Cabibbo Giuseppe, Celsa Ciro, Enea Marco, Battaglia Salvatore, Rizzo Giacomo Emanuele Maria, Grimaudo Stefania, Matranga Domenica, Attanasio Massimo, Bruzzi Paolo, Craxì Antonio, Cammà Calogero
Department of Health Promotion Sciences Maternal and Infant Care, Section of Gastroenterology & Hepatology, Internal Medicine and Medical Specialties, PROMISE, University of Palermo, 90127 Palermo, Italy.
Department of Surgical, Oncological and Oral Sciences (Di.Chir.On.S.), University of Palermo, 90127 Palermo, Italy.
Cancers (Basel). 2020 Jul 31;12(8):2132. doi: 10.3390/cancers12082132.
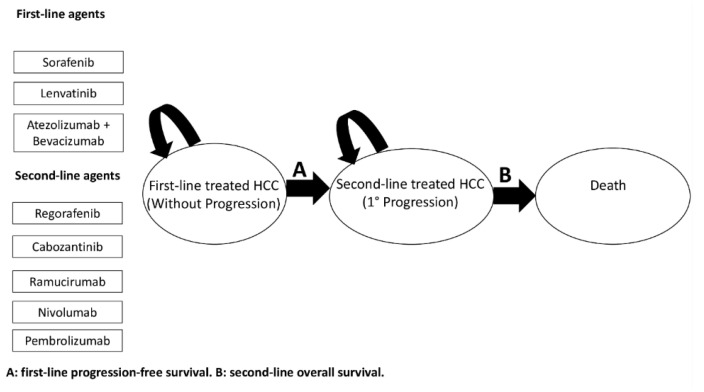
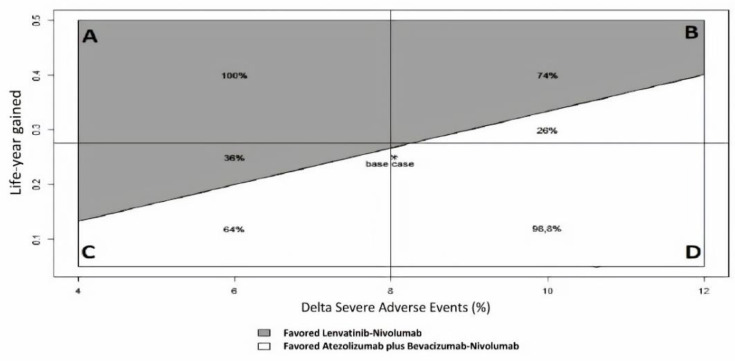
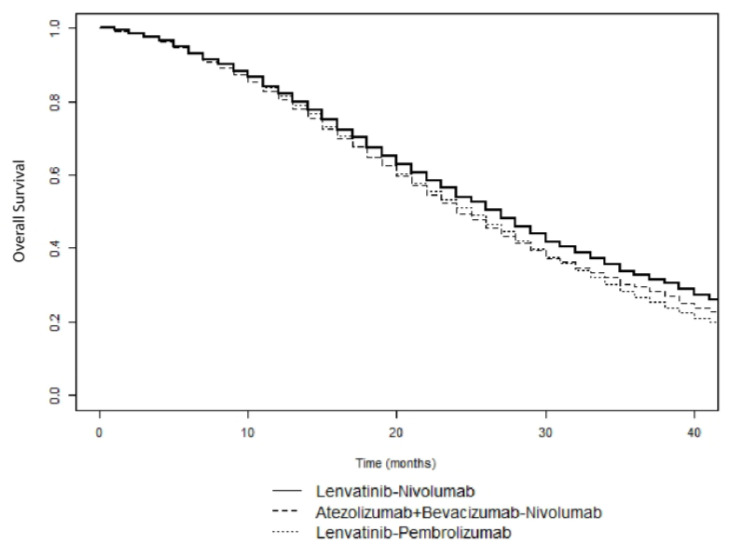
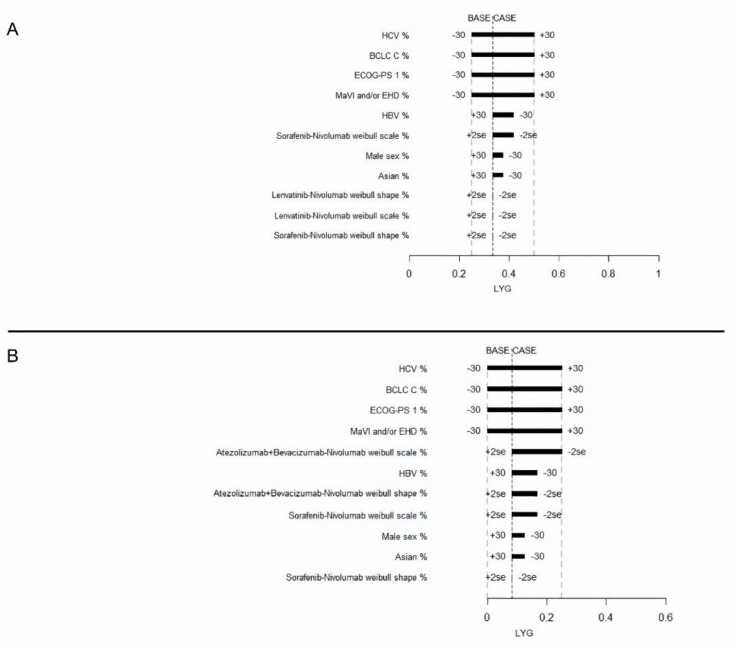
An optimal sequential systemic therapy for advanced hepatocellular carcinoma (HCC) has not been discovered. We developed a decision model based on available clinical trials to identify an optimal risk/benefit strategy for sequences of novel systemic agents. A Markov model was built to simulate overall survival (OS) among patients with advanced HCC. Three first-line (single-agent Sorafenib or Lenvatinib, and combination of Atezolizumab plus Bevacizumab) followed by five second-line treatments (Regorafenib, Cabozantinib, Ramucirumab, Nivolumab, Pembrolizumab) were compared in fifteen sequential strategies. The likelihood of transition between states (initial treatment, cancer progression, death) was derived from clinical trials. Life-year gained (LYG) was the main outcome. Rates of severe adverse events (SAEs) (≥grade 3) were calculated. The innovative measure, called incremental safety-effectiveness ratio (ISER), of the two best sequential treatments was calculated as the difference in probability of SAEs divided by LYG. Lenvatinib followed by Nivolumab (median OS, 27 months) was the most effective sequence, producing a LYG of 0.75, while Atezolizumab plus Bevacizumab followed by Nivolumab was the safest sequence (SAEs 40%). Accordingly, the net health benefit assessed by ISER favored Lenvatinib followed by Nivolumab, compared to Atezolizumab plus Bevacizumab, followed by Nivolumab in 52% of cases. : Further sequential clinical trials or large-scale real-world studies may prove useful to evaluate the net health benefit of the best sequential treatment for advanced HCC.
尚未发现针对晚期肝细胞癌(HCC)的最佳序贯全身治疗方案。我们基于现有临床试验开发了一个决策模型,以确定新型全身治疗药物序列的最佳风险/获益策略。构建了一个马尔可夫模型来模拟晚期HCC患者的总生存期(OS)。在15种序贯策略中比较了三种一线治疗方案(单药索拉非尼或仑伐替尼,以及阿替利珠单抗联合贝伐单抗),随后是五种二线治疗方案(瑞戈非尼、卡博替尼、雷莫西尤单抗、纳武利尤单抗、帕博利珠单抗)。状态之间转换(初始治疗、癌症进展、死亡)的可能性来自临床试验。获得的生命年(LYG)是主要结果。计算了严重不良事件(SAEs)(≥3级)的发生率。计算了两种最佳序贯治疗方案的创新指标,即增量安全有效性比(ISER),计算方法为SAEs概率的差异除以LYG。仑伐替尼序贯纳武利尤单抗(中位OS,27个月)是最有效的序列,LYG为0.75,而阿替利珠单抗联合贝伐单抗序贯纳武利尤单抗是最安全的序列(SAEs发生率40%)。因此,通过ISER评估的净健康效益在52%的情况下支持仑伐替尼序贯纳武利尤单抗,而不是阿替利珠单抗联合贝伐单抗序贯纳武利尤单抗。进一步的序贯临床试验或大规模真实世界研究可能有助于评估晚期HCC最佳序贯治疗的净健康效益。