Division of Rheumatology, Department of Medicine, University of California, Los Angeles, Los Angeles, CA.
Division of Rheumatology, Department of Medicine, University of Washington, Seattle, WA, USA.
Rheumatology (Oxford). 2022 Apr 11;61(4):1385-1395. doi: 10.1093/rheumatology/keab460.
To compare the safety and efficacy of switching from reference adalimumab to adalimumab biosimilar CT-P17 with continuing reference adalimumab/CT-P17 in active RA.
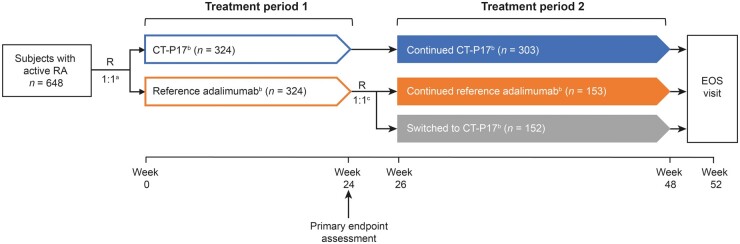
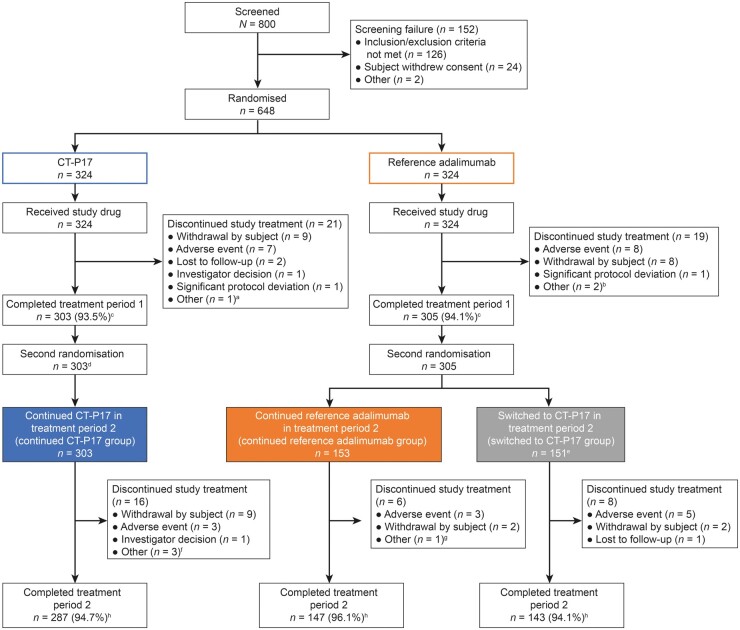
This double-blind, phase III study randomized (1:1) subjects with active RA to receive 40 mg (100 mg/ml) CT-P17 or European Union-sourced reference adalimumab subcutaneously every 2 weeks (Q2W) until week (W) 24 [treatment period (TP) 1]. Thereafter, subjects receiving reference adalimumab were randomized (1:1) to continue reference adalimumab or switch to CT-P17 from W26 (both Q2W until W48; TP2). Subjects receiving CT-P17 in TP1 continued CT-P17. W0-W24 results were previously reported; we present W26-W52 findings. End points were efficacy (including joint damage progression), pharmacokinetics, safety and immunogenicity.
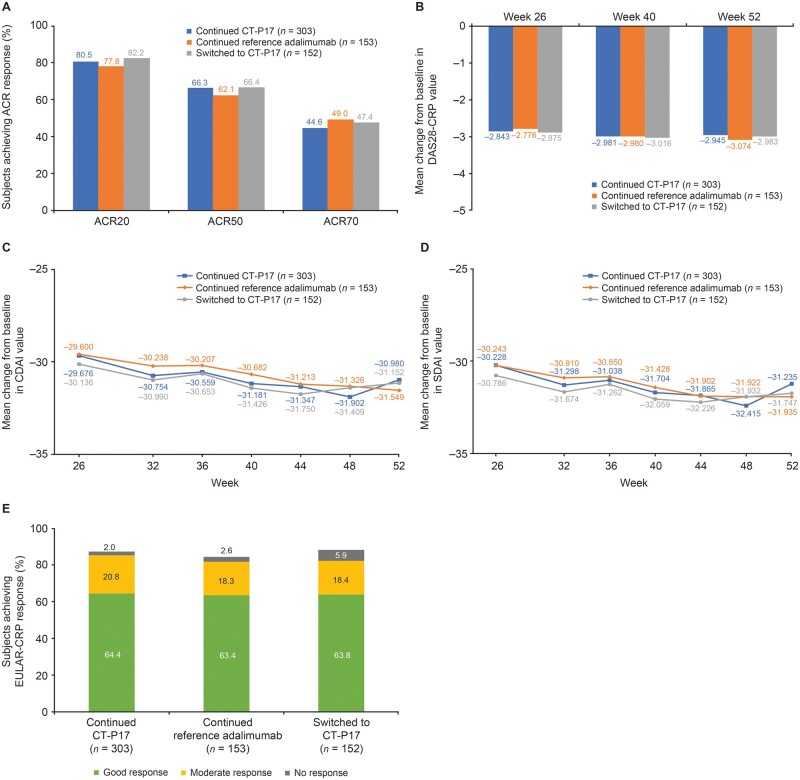
Of 607 subjects who initiated TP2 treatment, 303 continued CT-P17, 153 continued reference adalimumab and 151 switched to CT-P17. Efficacy improvements up to W24 were maintained during TP2; efficacy was comparable among groups. At W52, 20% improvement in ACR response rates were 80.5% (continued CT-P17), 77.8% (continued reference adalimumab) and 82.2% (switched to CT-P17). Joint damage progression was minimal. Mean trough serum adalimumab concentrations were similar among groups. CT-P17 and reference adalimumab safety profiles were numerically similar and switching did not affect immunogenicity. At W52, 28.4% (continued CT-P17), 27.0% (continued reference adalimumab) and 28.3% (switched to CT-P17) of subjects were anti-drug antibody-positive.
Efficacy, pharmacokinetics, safety and immunogenicity of CT-P17 and reference adalimumab were comparable after 1 year of treatment, including after switching from reference adalimumab to CT-P17.
ClinicalTrials.gov, http://clinicaltrials.gov, NCT03789292.
比较从参考阿达木单抗转换为阿达木单抗生物类似药 CT-P17 与继续使用参考阿达木单抗/CT-P17 治疗活动性 RA 的安全性和疗效。
这项双盲、III 期研究将活动性 RA 受试者(1:1)随机分为皮下注射 40mg(100mg/ml)CT-P17 或欧盟来源的参考阿达木单抗,每 2 周(Q2W)一次,直至第 24 周(治疗期 1[TP1])。此后,接受参考阿达木单抗的受试者(1:1)随机分为继续接受参考阿达木单抗或从第 26 周(均 Q2W 至第 48 周;TP2)转换为 CT-P17。在 TP1 中接受 CT-P17 的受试者继续接受 CT-P17。之前报告了第 0 至 24 周的结果;我们介绍第 26 至 52 周的结果。终点为疗效(包括关节损伤进展)、药代动力学、安全性和免疫原性。
在开始 TP2 治疗的 607 名受试者中,303 名继续接受 CT-P17 治疗,153 名继续接受参考阿达木单抗治疗,151 名转换为 CT-P17 治疗。在 TP2 期间,第 24 周的疗效改善得以维持;各组间疗效相当。在第 52 周时,ACR 反应率改善 20%的比例分别为 80.5%(继续接受 CT-P17)、77.8%(继续接受参考阿达木单抗)和 82.2%(转换为 CT-P17)。关节损伤进展最小。各组间平均血清阿达木单抗浓度相似。CT-P17 和参考阿达木单抗的安全性概况在数值上相似,转换并未影响免疫原性。在第 52 周时,继续接受 CT-P17 的受试者中有 28.4%(28.4%)、继续接受参考阿达木单抗的受试者中有 27.0%(27.0%)和转换为 CT-P17 的受试者中有 28.3%(28.3%)为抗药物抗体阳性。
在治疗 1 年后,CT-P17 和参考阿达木单抗的疗效、药代动力学、安全性和免疫原性相当,包括从参考阿达木单抗转换为 CT-P17 后。
ClinicalTrials.gov,http://clinicaltrials.gov,NCT03789292。