Safarika Asimina, Wacker James W, Katsaros Konstantinos, Solomonidi Nicky, Giannikopoulos George, Kotsaki Antigone, Koutelidakis Ioannis M, Coyle Sabrina M, Cheng Henry K, Liesenfeld Oliver, Sweeney Timothy E, Giamarellos-Bourboulis Evangelos J
4th Department of Internal Medicine, National and Kapodistrian University of Athens, ATTIKON University Hospital, 1 Rimini Str, 12462, Athens, Greece.
Inflammatix Inc, Clinical Affairs, Burlingame, CA, USA.
Intensive Care Med Exp. 2021 Jun 18;9(1):31. doi: 10.1186/s40635-021-00394-8.
Whether or not to administer antibiotics is a common and challenging clinical decision in patients with suspected infections presenting to the emergency department (ED). We prospectively validate InSep, a 29-mRNA blood-based host response test for the prediction of bacterial and viral infections.
The PROMPT trial is a prospective, non-interventional, multi-center clinical study that enrolled 397 adult patients presenting to the ED with signs of acute infection and at least one vital sign change. The infection status was adjudicated using chart review (including a syndromic molecular respiratory panel, procalcitonin and C-reactive protein) by three infectious disease physicians blinded to InSep results. InSep (version BVN-2) was performed using PAXgene Blood RNA processed and quantified on NanoString nCounter SPRINT. InSep results (likelihood of bacterial and viral infection) were compared to the adjudicated infection status.
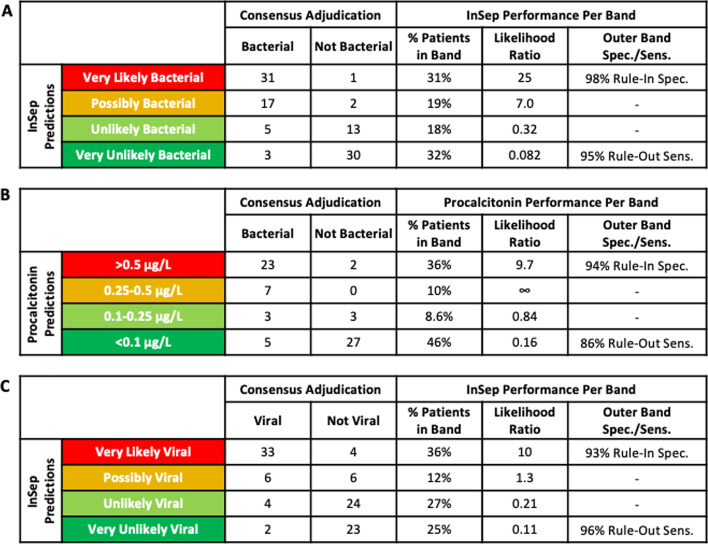
Subject mean age was 64 years, comorbidities were significant for diabetes (17.1%), chronic obstructive pulmonary disease (13.6%), and severe neurological disease (6.8%); 16.9% of subjects were immunocompromised. Infections were adjudicated as bacterial (14.1%), viral (11.3%) and noninfected (0.25%): 74.1% of subjects were adjudicated as indeterminate. InSep distinguished bacterial vs. viral/noninfected patients and viral vs. bacterial/noninfected patients using consensus adjudication with AUROCs of 0.94 (95% CI 0.90-0.99) and 0.90 (95% CI 0.83-0.96), respectively. AUROCs for bacterial vs. viral/noninfected patients were 0.88 (95% CI 0.79-0.96) for PCT, 0.80 (95% CI 0.72-89) for CRP and 0.78 (95% CI 0.69-0.87) for white blood cell counts (of note, the latter biomarkers were provided as part of clinical adjudication). To enable clinical actionability, InSep incorporates score cutoffs to allocate patients into interpretation bands. The Very Likely (rule in) InSep bacterial band showed a specificity of 98% compared to 94% for the corresponding PCT band (> 0.5 µg/L); the Very Unlikely (rule-out) band showed a sensitivity of 95% for InSep compared to 86% for PCT. For the detection of viral infections, InSep demonstrated a specificity of 93% for the Very Likely band (rule in) and a sensitivity of 96% for the Very Unlikely band (rule out).
InSep demonstrated high accuracy for predicting the presence of both bacterial and viral infections in ED patients with suspected acute infections or suspected sepsis. When translated into a rapid, point-of-care test, InSep will provide ED physicians with actionable results supporting early informed treatment decisions to improve patient outcomes while upholding antimicrobial stewardship. Registration number at Clinicaltrials.gov NCT03295825.
对于前往急诊科(ED)就诊的疑似感染患者,是否使用抗生素是一个常见且具有挑战性的临床决策。我们前瞻性地验证了InSep,这是一种基于29种mRNA的血液宿主反应检测方法,用于预测细菌和病毒感染。
PROMPT试验是一项前瞻性、非干预性、多中心临床研究,纳入了397名因急性感染体征和至少一项生命体征变化而前往急诊科就诊的成年患者。由三名对InSep结果不知情的传染病医生通过病历审查(包括综合征分子呼吸检测、降钙素原和C反应蛋白)来判定感染状态。使用在NanoString nCounter SPRINT上处理和定量的PAXgene Blood RNA进行InSep(BVN - 2版本)检测。将InSep结果(细菌和病毒感染的可能性)与判定的感染状态进行比较。
受试者的平均年龄为64岁,合并症在糖尿病(17.1%)、慢性阻塞性肺疾病(13.6%)和严重神经系统疾病(6. [此处原文有误,应为6.8%])中较为显著;16.9%的受试者存在免疫功能低下。感染被判定为细菌感染(14.1%)、病毒感染(11.3%)和未感染(0.25%):74.1%的受试者被判定为不确定。InSep使用一致性判定区分细菌感染与病毒/未感染患者以及病毒感染与细菌/未感染患者,其曲线下面积(AUROC)分别为0.94(95%置信区间0.90 - 0.99)和0.90(95%置信区间0.83 - 0.96)。降钙素原(PCT)检测细菌感染与病毒/未感染患者的AUROC为0.88(95%置信区间0.79 - 0.96),C反应蛋白(CRP)为0.80(95%置信区间0.72 - 0.89),白细胞计数为0.78(95%置信区间0.69 - 0.87)(值得注意的是,后几种生物标志物是作为临床判定的一部分提供的)。为了实现临床可操作性,InSep纳入了分数截断值,将患者分配到不同的解读类别。InSep细菌感染的“极有可能(确诊)”类别与相应的PCT类别(>0.5μg/L)相比,特异性为98%,而PCT为94%;“极不可能(排除)”类别中,InSep的敏感性为95%,PCT为86%。对于病毒感染的检测,InSep“极有可能(确诊)”类别的特异性为93%,“极不可能(排除)”类别的敏感性为96%。
InSep在预测疑似急性感染或疑似脓毒症的急诊科患者中细菌和病毒感染的存在方面显示出高准确性。当转化为快速即时检测时,InSep将为急诊科医生提供可操作的结果,支持早期明智的治疗决策,以改善患者预后,同时坚持抗菌药物管理。Clinicaltrials.gov注册号:NCT03295825。