Department of Anaesthesia, Intensive Care and Pain Medicine, Division of Population Medicine, Cardiff University, UHW B Block 3, Heath Park Campus, Cardiff, CF14 4XN, UK.
Critical Care Directorate, Grange University Hospital, Aneurin Bevan University Health Board, Cwmbran, UK.
Sci Rep. 2021 Jun 28;11(1):13407. doi: 10.1038/s41598-021-92874-w.
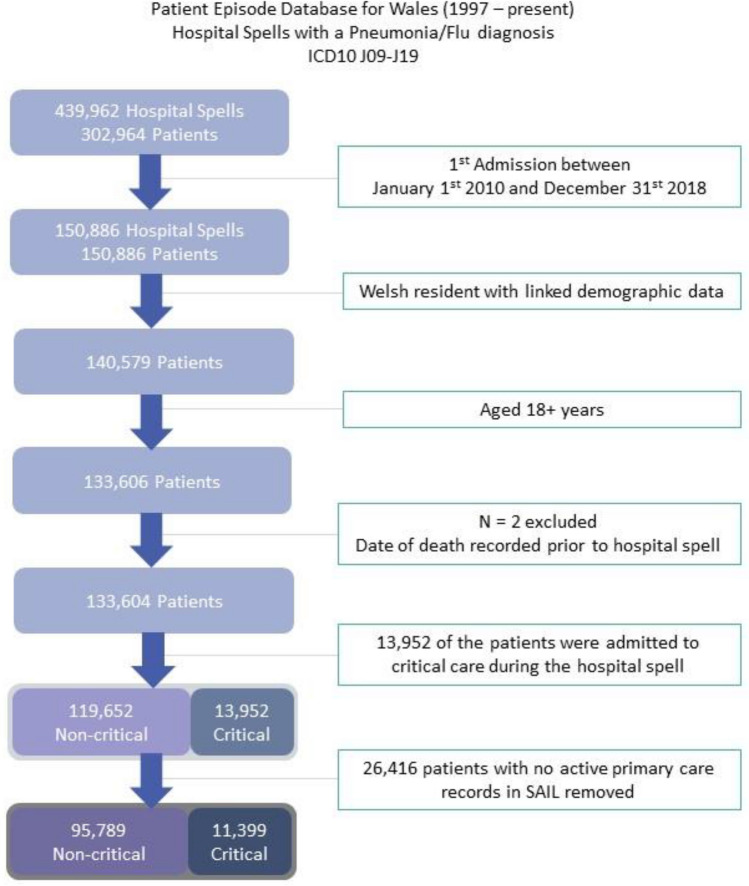
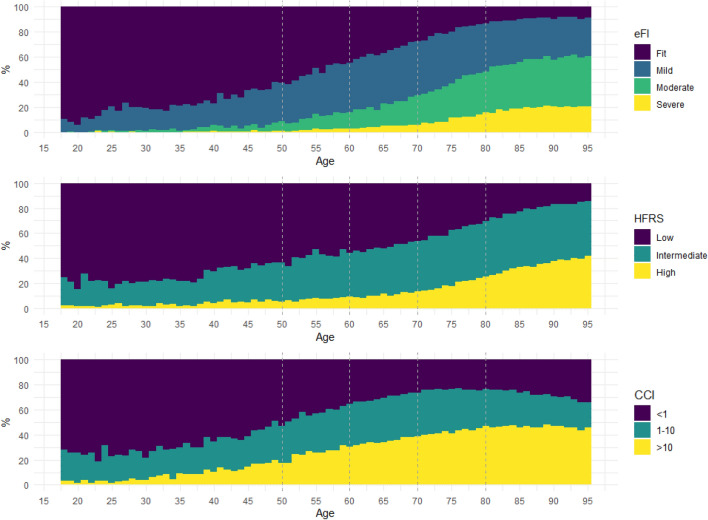
The ideal method of identifying frailty is uncertain, and data on long-term outcomes is relatively limited. We examined frailty indices derived from population-scale linked data on Intensive Care Unit (ICU) and hospitalised non-ICU patients with pneumonia to elucidate the influence of frailty on mortality. Longitudinal cohort study between 2010-2018 using population-scale anonymised data linkage of healthcare records for adults admitted to hospital with pneumonia in Wales. Primary outcome was in-patient mortality. Odds Ratios (ORs [95% confidence interval]) for age, hospital frailty risk score (HFRS), electronic frailty index (eFI), Charlson comorbidity index (CCI), and social deprivation index were estimated using multivariate logistic regression models. The area under the receiver operating characteristic curve (AUC) was estimated to determine the best fitting models. Of the 107,188 patients, mean (SD) age was 72.6 (16.6) years, 50% were men. The models adjusted for the two frailty indices and the comorbidity index had an increased odds of in-patient mortality for individuals with an ICU admission (ORs for ICU admission in the eFI model 2.67 [2.55, 2.79], HFRS model 2.30 [2.20, 2.41], CCI model 2.62 [2.51, 2.75]). Models indicated advancing age, increased frailty and comorbidity were also associated with an increased odds of in-patient mortality (eFI, baseline fit, ORs: mild 1.09 [1.04, 1.13], moderate 1.13 [1.08, 1.18], severe 1.17 [1.10, 1.23]. HFRS, baseline low, ORs: intermediate 2.65 [2.55, 2.75], high 3.31 [3.17, 3.45]). CCI, baseline < 1, ORs: '1-10' 1.15 [1.11, 1.20], > 10 2.50 [2.41, 2.60]). For predicting inpatient deaths, the CCI and HFRS based models were similar, however for longer term outcomes the CCI based model was superior. Frailty and comorbidity are significant risk factors for patients admitted to hospital with pneumonia. Frailty and comorbidity scores based on administrative data have only moderate ability to predict outcome.
确定脆弱性的理想方法不确定,关于长期结果的数据相对有限。我们研究了从人群规模的 ICU 和住院非 ICU 肺炎患者的相关数据中得出的脆弱性指数,以阐明脆弱性对死亡率的影响。这是一项 2010-2018 年期间的纵向队列研究,使用人群规模的威尔士住院肺炎患者医疗记录的匿名数据链接进行。主要结局是住院死亡率。使用多变量逻辑回归模型估计年龄、医院脆弱性风险评分 (HFRS)、电子脆弱性指数 (eFI)、Charlson 合并症指数 (CCI) 和社会剥夺指数的优势比 (OR [95%置信区间])。估计受试者工作特征曲线下的面积 (AUC) 以确定最佳拟合模型。在 107188 名患者中,平均 (SD) 年龄为 72.6 (16.6) 岁,50%为男性。调整了两个脆弱性指数和合并症指数的模型显示,入住 ICU 的个体住院死亡率的几率增加(eFI 模型的 ICU 入住率为 2.67 [2.55, 2.79],HFRS 模型为 2.30 [2.20, 2.41],CCI 模型为 2.62 [2.51, 2.75])。模型表明,年龄增长、脆弱性增加和合并症与住院死亡率增加也有关(eFI,基线拟合,ORs:轻度 1.09 [1.04, 1.13],中度 1.13 [1.08, 1.18],重度 1.17 [1.10, 1.23]。HFRS,基线低,ORs:中度 2.65 [2.55, 2.75],高 3.31 [3.17, 3.45])。CCI,基线 < 1,ORs:'1-10' 1.15 [1.11, 1.20], > 10 2.50 [2.41, 2.60])。对于预测住院死亡,CCI 和 HFRS 为基础的模型相似,但对于长期结果,基于 CCI 的模型更好。脆弱性和合并症是肺炎住院患者的重要危险因素。基于行政数据的脆弱性和合并症评分仅能适度预测结局。