Department of Anesthesiology, Shanghai First Maternity and Infant Hospital, Tongji University School of Medicine, No. 2699 W Gaoke Rd, Shanghai, 201024, China.
Department of Statistics and Data Management, Children's Hospital of Fudan University, No. 399 Wanyuan Rd, Shanghai, 201102, China.
BMC Pregnancy Childbirth. 2021 Jun 29;21(1):464. doi: 10.1186/s12884-021-03925-z.
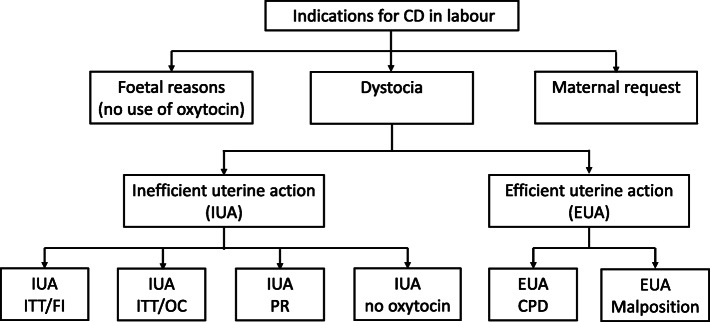
In this study, we aimed to determine whether epidural analgesia affects the indications for intrapartum caesarean delivery, such as foetal distress, dystocia, or maternal request, in nulliparous term women with spontaneous labour (Group 1 in the 10-Group Classification System).
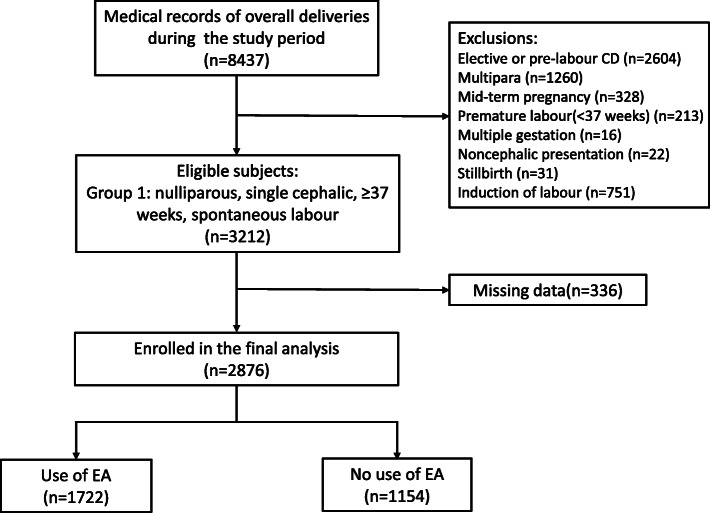
We conducted a retrospective cohort study and collected data from the electronic medical records of deliveries performed in our institution between 1 January 2017 and 30 June 2017. Women conforming to the criterion of Group 1 according to the 10-Group Classification System were enrolled. We compared labour outcomes between women with and without epidural analgesia and analysed the association between epidural analgesia and indications for caesarean by using multivariate logistic regression analysis.
A total of 3212 women met the inclusion criteria, and 2876 were enrolled in the final analyses. Women who received epidural analgesia had a significantly lower intrapartum caesarean delivery rate (16.0% vs. 26.7%, P < 0.001), higher rates of amniotomy (53.4% vs. 42.3%, P < 0.001) and oxytocin augmentation (79.5% vs. 67.0%, P < 0.001), and a higher incidence of intrapartum fever (≥38 °C) (23.3% vs. 8.5%, P < 0.001) than those who did not receive epidural analgesia. There were no significant differences between the groups for most indications, except a lower probability of maternal request for caesarean delivery (3.9% vs. 10.5%, P < 0.001) observed in women who received epidural analgesia than in those who did not. Epidural analgesia was revealed to be associated with a decreased risk of maternal request for caesarean delivery (adjusted odds ratio [aOR], 0.30; 95% confidence interval [CI], 0.22-0.42; P < 0.001); however, oxytocin augmentation was related to an increased risk of maternal request (aOR, 2.34; 95%CI, 1.47-3.75; P < 0.001). Regarding the reasons for the maternal request for caesarean delivery, significantly fewer women complained of pain (0.5% vs. 4.6%, P < 0.001) or had no labour progress (1.3% vs. 3.6%, P < 0.001) among those who received analgesia.
Among the women in Group 1, epidural analgesia was associated with a lower intrapartum caesarean delivery rate, which may be explained by a reduction in the risk of maternal request for an intrapartum caesarean delivery.
本研究旨在探讨硬膜外镇痛是否会影响产程中剖宫产的指征,如胎儿窘迫、产程延长或产妇要求,在自发性分娩的初产妇(10 分组分类系统中的第 1 组)中。
我们进行了一项回顾性队列研究,收集了 2017 年 1 月 1 日至 6 月 30 日期间我院分娩的电子病历数据。根据 10 分组分类系统,符合第 1 组标准的女性被纳入研究。我们比较了接受和未接受硬膜外镇痛的产妇的分娩结局,并使用多变量逻辑回归分析了硬膜外镇痛与剖宫产指征之间的关系。
共有 3212 名女性符合纳入标准,最终有 2876 名女性纳入最终分析。接受硬膜外镇痛的女性剖宫产率显著降低(16.0% vs. 26.7%,P<0.001),行人工破膜(53.4% vs. 42.3%,P<0.001)和缩宫素催引产(79.5% vs. 67.0%,P<0.001)的比例更高,产时发热(≥38℃)的发生率(23.3% vs. 8.5%,P<0.001)更高。除了接受硬膜外镇痛的产妇中因产妇要求行剖宫产的比例较低(3.9% vs. 10.5%,P<0.001)外,两组在大多数指征上无显著差异。硬膜外镇痛与因产妇要求行剖宫产的风险降低相关(调整优势比[aOR],0.30;95%置信区间[CI],0.22-0.42;P<0.001);然而,缩宫素催引产与因产妇要求行剖宫产的风险增加相关(aOR,2.34;95%CI,1.47-3.75;P<0.001)。关于因产妇要求行剖宫产的原因,接受镇痛的产妇中,疼痛(0.5% vs. 4.6%,P<0.001)或产程无进展(1.3% vs. 3.6%,P<0.001)的抱怨明显减少。
在第 1 组产妇中,硬膜外镇痛与剖宫产率降低相关,这可能是由于因产妇要求行剖宫产的风险降低所致。