Department of Cardiology, Third Xiangya Hospital, Central South University, Changsha, Hunan, China.
Clinical Research Center, Third Xiangya Hospital, Central South University, Changsha, Hunan, China.
BMJ Open. 2021 Jun 29;11(6):e044072. doi: 10.1136/bmjopen-2020-044072.
The survival benefit of using mechanical circulatory support (MCS) in patients with acute myocardial infarction (AMI) is still controversial. It is necessary to explore the impact on clinical outcomes of MCS in patients with AMI undergoing stenting.
Systematic review and meta-analysis.
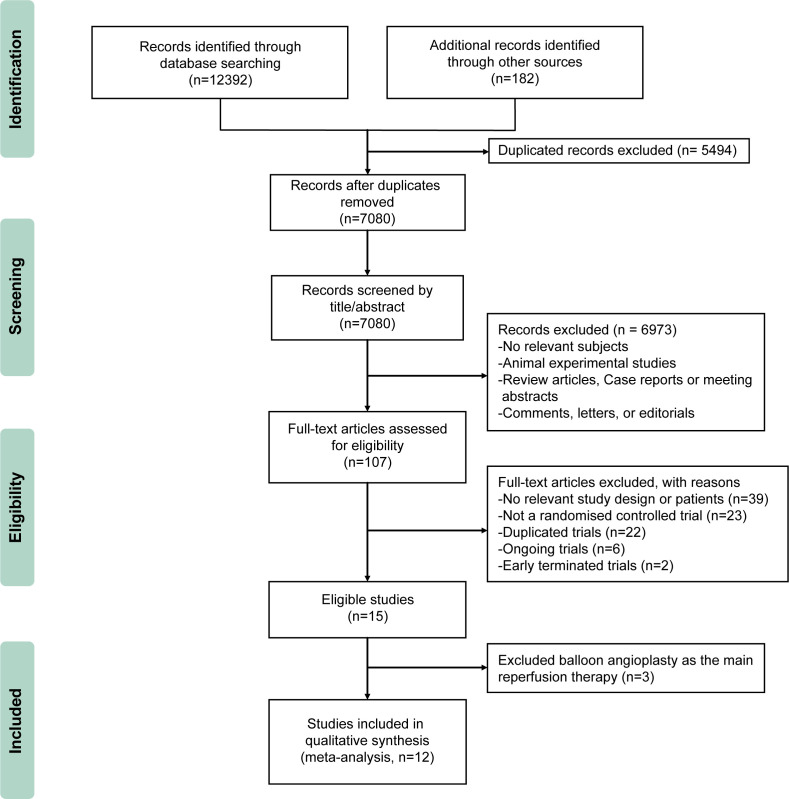
Embase, Cochrane Library, Medline, PubMed, Web of Science, ClinicalTrials.gov and Clinicaltrialsregister.eu databases were searched from database inception to February 2021.
Randomised clinical trials (RCTs) on MCS use in patients with AMI undergoing stent implantation were included.
Data were extracted and summarised independently by two reviewers. Risk ratios (RRs) and 95% CIs were calculated for clinical outcomes according to random-effects model.
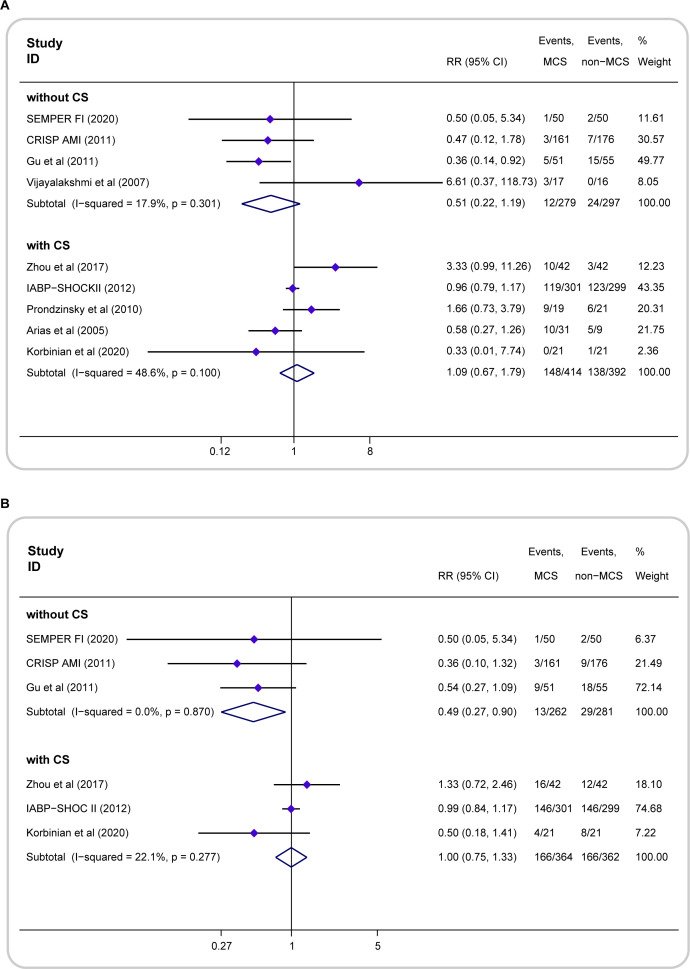
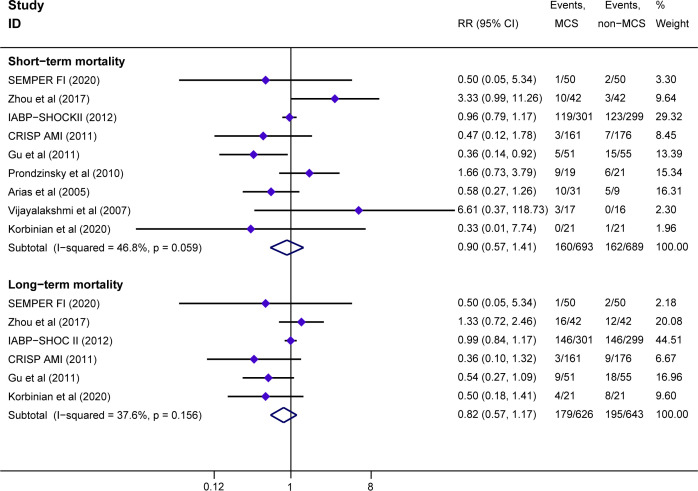
Twelve studies of 1497 patients with AMI were included, nine studies including 1382 patients compared MCS with non-MCS, and three studies including 115 patients compared percutaneous ventricular assist devices (pVADs) versus intra-aortic balloon pump (IABP). Compared with non-MCS, MCS was not associated with short-term (within 30 days) (RR=0.90; 95% CI 0.57 to 1.41; I=46.8%) and long-term (at least 6 months) (RR=0.82; 95% CI 0.57 to 1.17; I=37.6%) mortality reductions. In the subset of patients without cardiogenic shock (CS) compared with non-MCS, the patients with IABP treatment significantly had decreased long-term mortality (RR=0.49; 95% CI 0.27 to 0.90; I=0), but without the short-term mortality reductions (RR=0.51; 95% CI 0.22 to 1.19; I=17.9%). While in the patients with CS, the patients with MCS did not benefit from the short-term (RR=1.09; 95% CI 0.67 to 1.79; I=46.6%) or long-term (RR=1.00; 95% CI 0.75 to 1.33; I=22.1%) survival. Moreover, the application of pVADs increased risk of bleeding (RR=1.86; 95% CI 1.15 to 3.00; I=15.3%) compared with IABP treatment (RR=1.86; 95% CI 1.15 to 3.00; I=15.3%).
In all patients with AMI undergoing stent implantation, the MCS use does not reduce all-cause mortality. Patients without CS can benefit from MCS regarding long-term survival, while patients with CS seem not.
使用机械循环支持(MCS)治疗急性心肌梗死(AMI)患者的生存获益仍存在争议。有必要探讨 MCS 对接受支架植入术的 AMI 患者临床结局的影响。
系统评价和荟萃分析。
从数据库建立到 2021 年 2 月,检索了 Embase、Cochrane 图书馆、Medline、PubMed、Web of Science、ClinicalTrials.gov 和 Clinicaltrialsregister.eu 数据库。
纳入了关于 AMI 患者接受支架植入术时使用 MCS 的随机临床试验(RCT)。
两名评审员独立提取和总结数据。根据随机效应模型计算临床结局的风险比(RR)和 95%置信区间(CI)。
纳入了 1497 例 AMI 患者的 12 项研究,9 项研究比较了 MCS 与非 MCS,3 项研究比较了经皮心室辅助装置(pVAD)与主动脉内球囊泵(IABP)。与非 MCS 相比,MCS 与短期(30 天内)(RR=0.90;95%CI 0.57 至 1.41;I=46.8%)和长期(至少 6 个月)(RR=0.82;95%CI 0.57 至 1.17;I=37.6%)死亡率降低无关。在无心源性休克(CS)的患者亚组中,与非 MCS 相比,IABP 治疗显著降低了长期死亡率(RR=0.49;95%CI 0.27 至 0.90;I=0),但短期死亡率没有降低(RR=0.51;95%CI 0.22 至 1.19;I=17.9%)。而在 CS 患者中,MCS 并不能从短期(RR=1.09;95%CI 0.67 至 1.79;I=46.6%)或长期(RR=1.00;95%CI 0.75 至 1.33;I=22.1%)生存中获益。此外,与 IABP 治疗相比,pVAD 的应用增加了出血风险(RR=1.86;95%CI 1.15 至 3.00;I=15.3%)(RR=1.86;95%CI 1.15 至 3.00;I=15.3%)。
在所有接受支架植入术的 AMI 患者中,MCS 的使用并不能降低全因死亡率。无 CS 的患者可从 MCS 中获益,延长长期生存,而 CS 患者似乎不能获益。