Department of Cardiology, Medical University of Graz, Graz, Austria.
Cardiovascular Perfusionists Department of Cardiac Surgery, Medical University of Graz, Graz, Austria.
Catheter Cardiovasc Interv. 2022 Sep;100(3):319-327. doi: 10.1002/ccd.30327. Epub 2022 Jul 13.
Cardiogenic shock (CS) is a hemodynamically complex multisystem syndrome associated with persistently high morbidity and mortality. As CS is characterized by progressive failure to provide adequate systemic perfusion, supporting end-organ perfusion using mechanical circulatory support (MCS) seems intriguing. Since most patients with CS present in the catheterization laboratory, percutaneously implantable systems have the widest adoption in the field. We evaluated feasibility, outcomes, and complications after the introduction of a full-percutaneous program for both the Impella CP device and venoarterial extracorporeal membrane oxygenator (VA-ECMO).
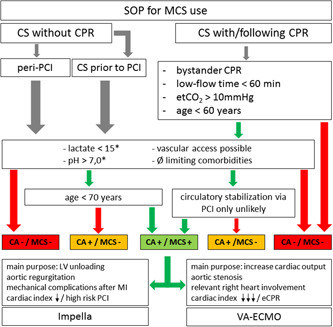
PREPARE CardShock (PRospective REgistry of PAtients in REfractory cardiogenic shock) is a prospective single-center registry, including 248 consecutive patients between May 2019 and April 2021, who underwent cardiac catheterization and displayed advanced cardiogenic shock. The median age was 70 (58-77) years and 28% were female. Sixty-five percent of the cases had cardiac arrest, of which 66% were out-of-hospital cardiac arrest. A local standard operating procedure (SOP) indicating indications as well as relative and absolute contraindications for different means of MCS (Impella CP or VA-ECMO) was used to guide MCS use. The primary endpoint was in-hospital death and secondary endpoints were spontaneous myocardial infarction and major bleedings during the hospital stay.
Overall mortality was 50.4% with a median survival of 2 (0-6) days. Significant independent predictors of mortality were cardiac arrest during the index event (odds ratio [OR] with 95% confidence interval [CI]: 2.53 [1.43-4.51]; p = 0.001), age > 65 years (OR: 2.05 [1.03-4.09]; p = 0.036]), pH < 7.30 (OR: 2.69 [1.56-4.66]; p < 0.001), and lactate levels > 2 mmol/L (OR: 4.51 [2.37-8.65]; p < 0.001).
Conclusive SOPs assist target-orientated MCS use in CS. This study provides guidance on the implementation, validation, and modification of newly established MCS programs to aid centers that are establishing such programs.
心源性休克(CS)是一种与持续高发病率和死亡率相关的血流动力学复杂的多系统综合征。由于 CS 的特征是持续存在全身灌注不足,因此使用机械循环支持(MCS)来支持终末器官灌注似乎很有吸引力。由于大多数 CS 患者在导管室就诊,因此经皮植入系统在该领域的应用最为广泛。我们评估了在引入 Impella CP 装置和静脉动脉体外膜肺氧合器(VA-ECMO)的全经皮治疗方案后,该方案的可行性、结果和并发症。
PREPARE CardShock(PRospective REgistry of PAtients in REfractory cardiogenic shock)是一项前瞻性单中心注册研究,纳入了 2019 年 5 月至 2021 年 4 月期间 248 例连续接受心脏导管检查并显示晚期心源性休克的患者。中位年龄为 70 岁(58-77 岁),28%为女性。65%的病例有心律失常,其中 66%为院外心脏骤停。使用当地的标准操作程序(SOP),指示不同 MCS 方法(Impella CP 或 VA-ECMO)的适应证和相对及绝对禁忌证,以指导 MCS 的使用。主要终点为住院期间死亡,次要终点为住院期间发生自发性心肌梗死和大出血。
总死亡率为 50.4%,中位生存时间为 2(0-6)天。死亡率的显著独立预测因素包括指数事件期间的心律失常(优势比[OR],95%置信区间[CI]:2.53[1.43-4.51];p=0.001)、年龄>65 岁(OR:2.05[1.03-4.09];p=0.036)、pH<7.30(OR:2.69[1.56-4.66];p<0.001)和乳酸水平>2mmol/L(OR:4.51[2.37-8.65];p<0.001)。
明确的 SOP 有助于 CS 中以目标为导向的 MCS 使用。本研究为新建立的 MCS 方案的实施、验证和修改提供了指导,以帮助正在建立此类方案的中心。