School of Physical Sciences, Dublin City University, Glasnevin, Dublin, Ireland.
Department of Oncology, University of Oxford, Oxford, United Kingdom.
JAMA Netw Open. 2021 Jun 1;4(6):e2115321. doi: 10.1001/jamanetworkopen.2021.15321.
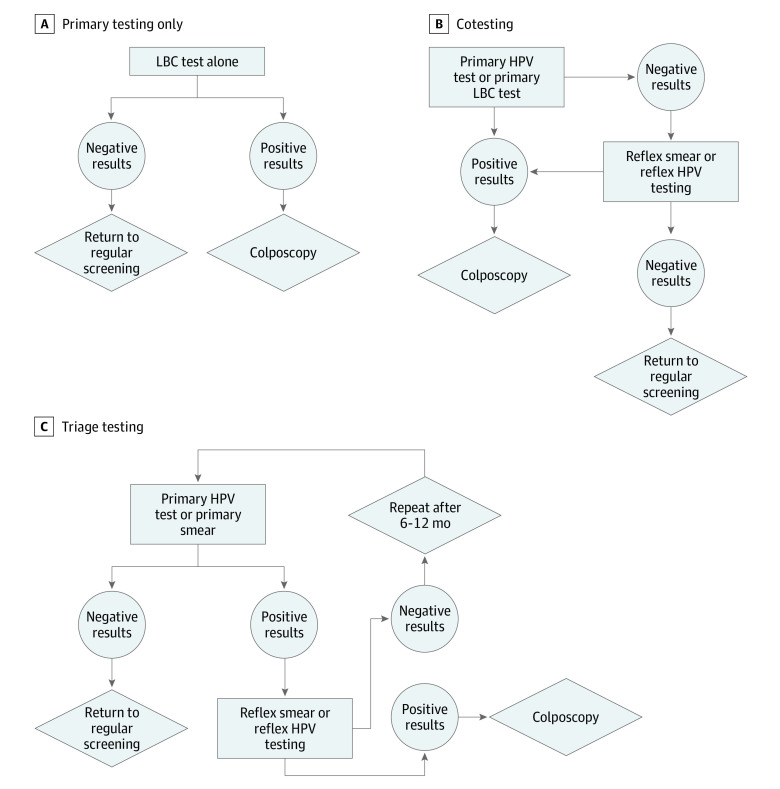
Cervical cancer screening is a lifesaving intervention, with an array of approaches, including liquid-based cytology (LBC), molecular testing for human papillomavirus (HPV) infection, and combinations via parallel cotesting or sequential triage. Maximizing screening efficacy while minimizing overtreatment is vital, especially when considering how the HPV vaccine will affect the interpretation of results.
To estimate the likely outcomes of different screening modalities and to model how the increasing uptake of the HPV vaccine could affect the interpretation of screening results.
DESIGN, SETTING, AND PARTICIPANTS: This decision analytic model established a simple Markov model to compare the outcomes of different cervical cancer screening modalities on a simulated population of women (aged ≥25 years), considering different levels of HPV vaccination.
The number of cases of cervical intraepithelial neoplasia (CIN) grade 2 and 3 detected and missed, the number of false positives, and the number of tests required to achieve a given level of accuracy. Positive and negative predictive values of different modalities were simulated under varying levels of HPV vaccination and therefore HPV prevalence.
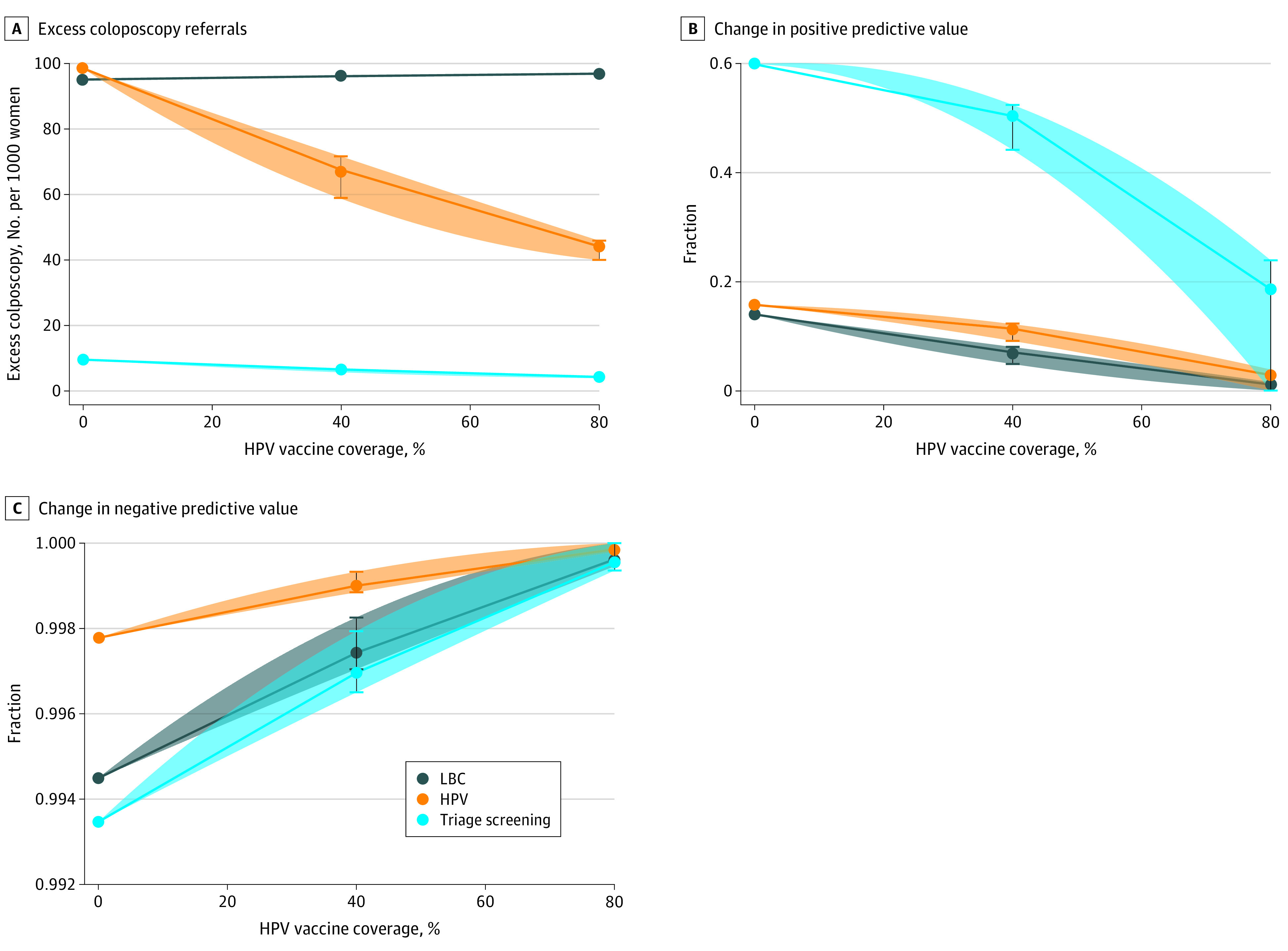
In a simulated population of 1000 women aged 25 years and older with an HPV prevalence of 2%, HPV-based modalities outperformed LBC-based approaches, detecting 19% more true positives (HPV test sensitivity, 89.9% [95% CI, 88.6%-91.1%]; LBC test sensitivity, 75.5% [95% CI, 66.6%-82.7%]). While cotesting markedly reduced missed cases, detecting 29% more true positives than LBC alone (19.5 [95% CI, 19.3-19.7] per 1000 women screened vs 15.1 [95% CI, 13.3-16.5] per 1000 women screened), it unacceptably increased excess colposcopy referral by 94% (184.4 [95% CI, 181.8-188.0] false positives per 1000 women screened vs 95.1 [95% CI, 93.1-97.0] false positives per 1000 women screened). By contrast, triage testing with reflex screening substantially reduced false positives by a factor of approximately 10 (eg, HPV with LBC triage, 9.6 [95% CI, 9.3-10.0] per 1000 women screened). Over a lifetime of screening, reflex approaches with appropriate test intervals maximized therapeutic efficacy; as HPV vaccination rates increased, HPV-based screening approaches resulted in fewer unnecessary colposcopies than LBC approaches (HPV testing, 80% vaccine coverage: 44.1 [95% CI, 40-45.9] excess colposcopies; LBC testing, 80% vaccine coverage: 96.9 [95% CI, 96.8-97.0] excess colposcopies).
In this decision analytic model, the effectiveness of cervical cancer screening was dependent on the prevalence of cervical dysplasia and/or HPV infection or vaccination in a population as well as the sensitivity and specificity of various modalities. Although screening is lifesaving, overtesting or modalities inappropriate to the target population may cause significant harm, including overtreatment.
宫颈癌筛查是一种拯救生命的干预措施,有多种方法,包括液基细胞学(LBC)、人乳头瘤病毒(HPV)感染的分子检测以及平行联合检测或顺序分流检测的组合。最大限度地提高筛查效果,同时最小化过度治疗至关重要,尤其是当考虑 HPV 疫苗将如何影响结果解释时。
估计不同筛查方式的可能结果,并建立模型以了解 HPV 疫苗接种率的增加如何影响筛查结果的解释。
设计、设置和参与者:本决策分析模型建立了一个简单的马尔可夫模型,以比较不同宫颈癌筛查方式在模拟人群(年龄≥25 岁)中的结果,同时考虑了 HPV 疫苗接种的不同水平。
检测和漏诊的宫颈上皮内瘤变(CIN)2 级和 3 级病例数、假阳性数以及实现特定准确性所需的检测次数。在不同 HPV 疫苗接种率和因此 HPV 流行率的情况下,模拟了不同方式的阳性和阴性预测值。
在一个模拟的 1000 名年龄在 25 岁及以上的女性人群中,HPV 流行率为 2%,基于 HPV 的方法优于基于 LBC 的方法,可检测出 19%更多的真阳性(HPV 检测敏感性为 89.9%[95%CI,88.6%-91.1%];LBC 检测敏感性为 75.5%[95%CI,66.6%-82.7%])。虽然联合检测显著减少了漏诊病例,与单独使用 LBC 相比,可检测出 29%更多的真阳性(19.5[95%CI,19.3-19.7]例/每 1000 名筛查女性与 15.1[95%CI,13.3-16.5]例/每 1000 名筛查女性),但它不可接受地将额外的阴道镜转诊增加了 94%(184.4[95%CI,181.8-188.0]例假阳性/每 1000 名筛查女性与 95.1[95%CI,93.1-97.0]例假阳性/每 1000 名筛查女性)。相比之下,通过 HPV 联合 LBC 进行分流检测可将假阳性率降低约 10 倍(例如,HPV 联合 LBC 分流检测,每 1000 名筛查女性中 9.6[95%CI,9.3-10.0]例假阳性)。在终生筛查中,适当的检测间隔的反射检测方法最大限度地提高了治疗效果;随着 HPV 疫苗接种率的提高,基于 HPV 的筛查方法导致不必要的阴道镜检查比基于 LBC 的方法少(HPV 检测,80%疫苗覆盖率:44.1[95%CI,40-45.9]例额外阴道镜检查;LBC 检测,80%疫苗覆盖率:96.9[95%CI,96.8-97.0]例额外阴道镜检查)。
在这个决策分析模型中,宫颈癌筛查的有效性取决于人群中宫颈发育不良和/或 HPV 感染或疫苗接种的流行率以及各种方法的敏感性和特异性。尽管筛查是救命的,但过度检测或不适合目标人群的方法可能会造成重大伤害,包括过度治疗。