Department of Pharmacy, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310009, China.
Department of Critical Care Medicine, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310009, China.
Antimicrob Resist Infect Control. 2021 Jun 30;10(1):98. doi: 10.1186/s13756-021-00969-w.
Infection is the leading cause of morbidity and mortality among burn patients, and bloodstream infection (BSI) is the most serious. This study aimed to evaluate the epidemiology and clinical outcomes of BSI in severe burn patients.
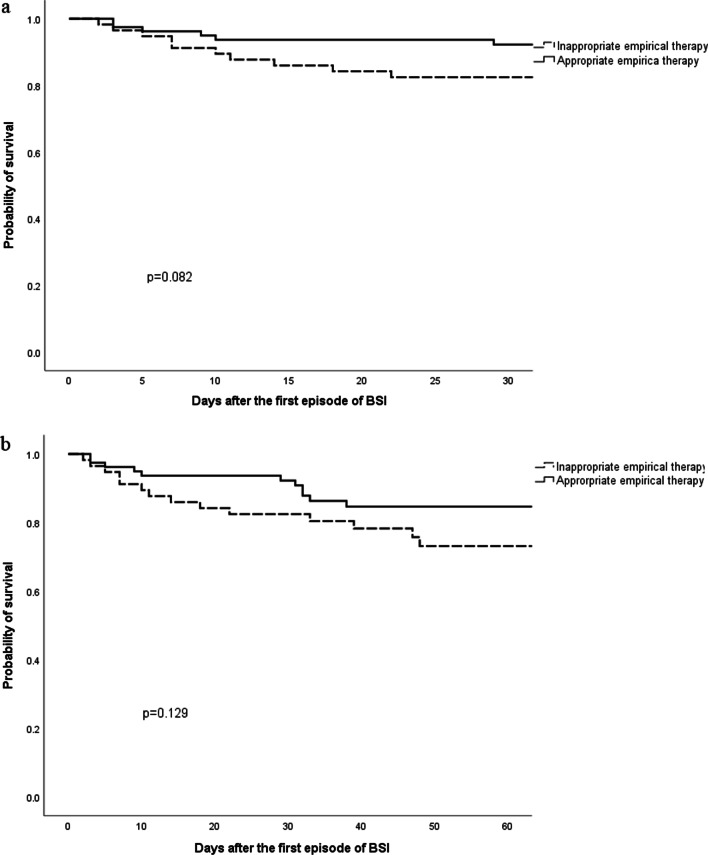
Clinical variables of all patients admitted with severe burns (≥ 20% total body surface area, %TBSA) were analyzed retrospectively from January 2013 to December 2018 at a teaching hospital. The Kaplan-Meier method was utilized for plotting survival curves. Multivariate logistic regression and Cox regression model were also performed.
A total of 495 patients were evaluated, of whom 136 (27.5%) had a BSI. The median time from the patients being burned to BSI was 8 days. For BSI onset in these patients, 47.8% (65/136) occurred in the first week. The most frequently isolated causative organism was A. baumannii (22.7%), followed by methicillin-resistant Staphylococcus aureus (18.7%) and K. pneumoniae (18.2%), in patients with BSI. Multivariate logistic regression analysis showed that %TBSA (p = 0.023), mechanical ventilation (p = 0.019), central venous catheter (CVC) (p < 0.001) and hospital length of stay (27d vs 50d, p < 0.001) were independent risk factors associated with BSI. Cox regression model showed that acute kidney injury (HR, 12.26; 95% CI 2.31-64.98; p = 0.003) and septic shock (HR, 4.36; 95% CI 1.16-16.34; p = 0.031) were identified as independent predictors of 30-day mortality of BSI in burn patients.
Multidrug resistant gram-negative bacteria were the main pathogens of BSI in severe burn patients. Accurate evaluation of risk factors for BSI and the mortality of BSI in severe burn patients may improve early appropriate management.
感染是烧伤患者发病率和死亡率的主要原因,血流感染(BSI)是最严重的感染。本研究旨在评估严重烧伤患者 BSI 的流行病学和临床结局。
回顾性分析 2013 年 1 月至 2018 年 12 月期间,一家教学医院收治的所有严重烧伤(≥20%总体表面积,%TBSA)患者的临床变量。采用 Kaplan-Meier 法绘制生存曲线。还进行了多变量逻辑回归和 Cox 回归模型分析。
共评估了 495 例患者,其中 136 例(27.5%)发生了 BSI。从烧伤到 BSI 的中位时间为 8 天。在这些患者中,BSI 发病的 47.8%(65/136)发生在第一周。BSI 患者中最常分离到的病原体是鲍曼不动杆菌(22.7%),其次是耐甲氧西林金黄色葡萄球菌(18.7%)和肺炎克雷伯菌(18.2%)。多变量逻辑回归分析表明,%TBSA(p=0.023)、机械通气(p=0.019)、中心静脉导管(CVC)(p<0.001)和住院时间(27d 与 50d,p<0.001)是与 BSI 相关的独立危险因素。Cox 回归模型显示,急性肾损伤(HR,12.26;95%CI,2.31-64.98;p=0.003)和感染性休克(HR,4.36;95%CI,1.16-16.34;p=0.031)是烧伤患者 BSI 30 天死亡率的独立预测因素。
多重耐药革兰氏阴性菌是严重烧伤患者 BSI 的主要病原体。准确评估 BSI 的危险因素和严重烧伤患者 BSI 的死亡率可能有助于改善早期的适当治疗。