Yalchin Mehmet, Baker Ann-Marie, Graham Trevor A, Hart Ailsa
Inflammatory Bowel Disease Department, St. Mark's Hospital, Watford R.d., Harrow HA1 3UJ, UK.
Centre for Genomics and Computational Biology, Barts Cancer Institute, Barts and the London School of Medicine and Dentistry, Queen Mary University of London, Charterhouse S.q., London EC1M 6BQ, UK.
Cancers (Basel). 2021 Jun 10;13(12):2908. doi: 10.3390/cancers13122908.
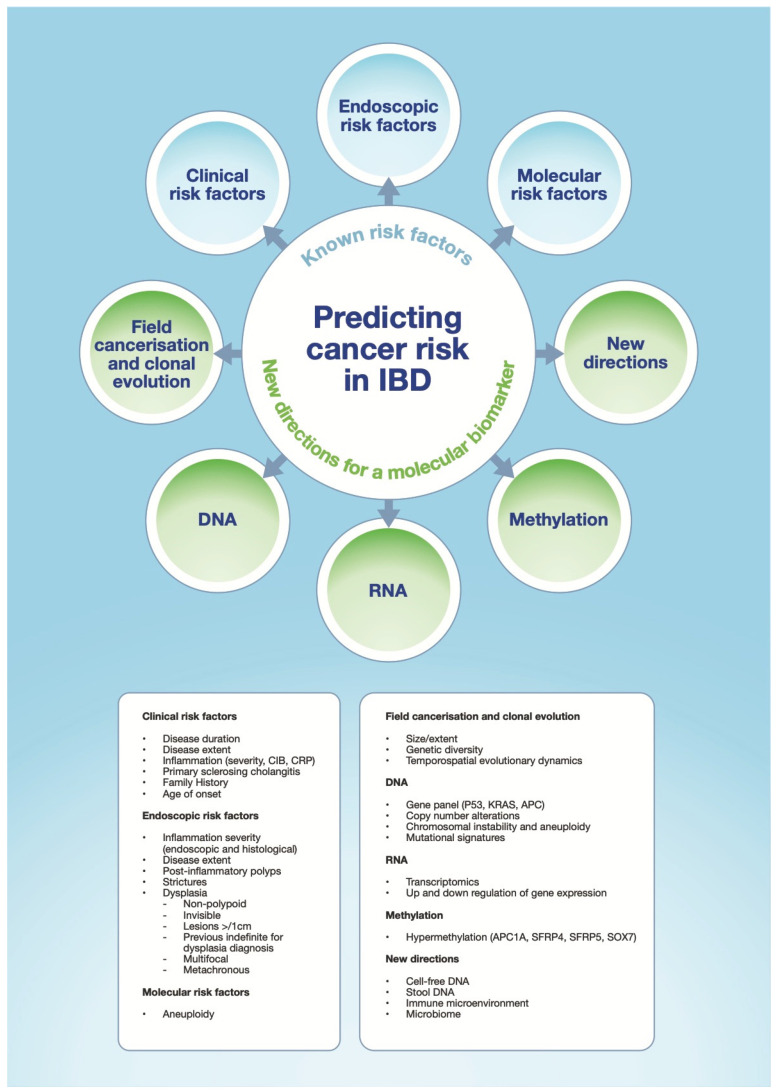
Patients with colonic inflammatory bowel disease (IBD) are at an increased risk of developing colorectal cancer (CRC), and are therefore enrolled into a surveillance programme aimed at detecting dysplasia or early cancer. Current surveillance programmes are guided by clinical, endoscopic or histological predictors of colitis-associated CRC (CA-CRC). We have seen great progress in our understanding of these predictors of disease progression, and advances in endoscopic technique and management, along with improved medical care, has been mirrored by the falling incidence of CA-CRC over the last 50 years. However, more could be done to improve our molecular understanding of CA-CRC progression and enable better risk stratification for patients with IBD. This review summarises the known risk factors associated with CA-CRC and explores the molecular landscape that has the potential to complement and optimise the existing IBD surveillance programme.
患有结肠炎症性肠病(IBD)的患者患结直肠癌(CRC)的风险增加,因此被纳入旨在检测发育异常或早期癌症的监测计划。目前的监测计划以结肠炎相关结直肠癌(CA-CRC)的临床、内镜或组织学预测指标为指导。我们在理解这些疾病进展预测指标方面取得了巨大进展,内镜技术和管理的进步,以及医疗护理的改善,反映在过去50年中CA-CRC发病率的下降。然而,在提高我们对CA-CRC进展的分子理解以及为IBD患者实现更好的风险分层方面,还有更多工作要做。本综述总结了与CA-CRC相关的已知风险因素,并探讨了有可能补充和优化现有IBD监测计划的分子格局。