GENUD Toledo Research Group, Universidad de Castilla-La Mancha, Toledo, Spain.
CIBER of Frailty and Healthy Aging (CIBERFES), Madrid, Spain.
J Cachexia Sarcopenia Muscle. 2021 Aug;12(4):921-932. doi: 10.1002/jcsm.12737. Epub 2021 Jul 3.
A validated, standardized, and feasible test to assess muscle power in older adults has recently been reported: the sit-to-stand (STS) muscle power test. This investigation aimed to assess the relationship between relative STS power and age and to provide normative data, cut-off points, and minimal clinically important differences (MCID) for STS power measures in older women and men.
A total of 9320 older adults (6161 women and 3159 men) aged 60-103 years and 586 young and middle-aged adults (318 women and 268 men) aged 20-60 years were included in this cross-sectional study. Relative (normalized to body mass), allometric (normalized to height squared), and specific (normalized to legs muscle mass) muscle power values were assessed by the 30 s STS power test. Body composition was evaluated by dual energy X-ray absorptiometry and bioelectrical impedance analysis, and legs skeletal muscle index (SMI; normalized to height squared) was calculated. Habitual and maximal gait speed, timed up-and-go test, and 6 min walking distance were collected as physical performance measures, and participants were classified into two groups: well-functioning and mobility-limited older adults.
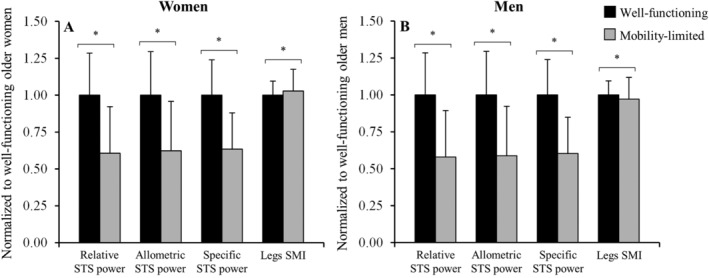
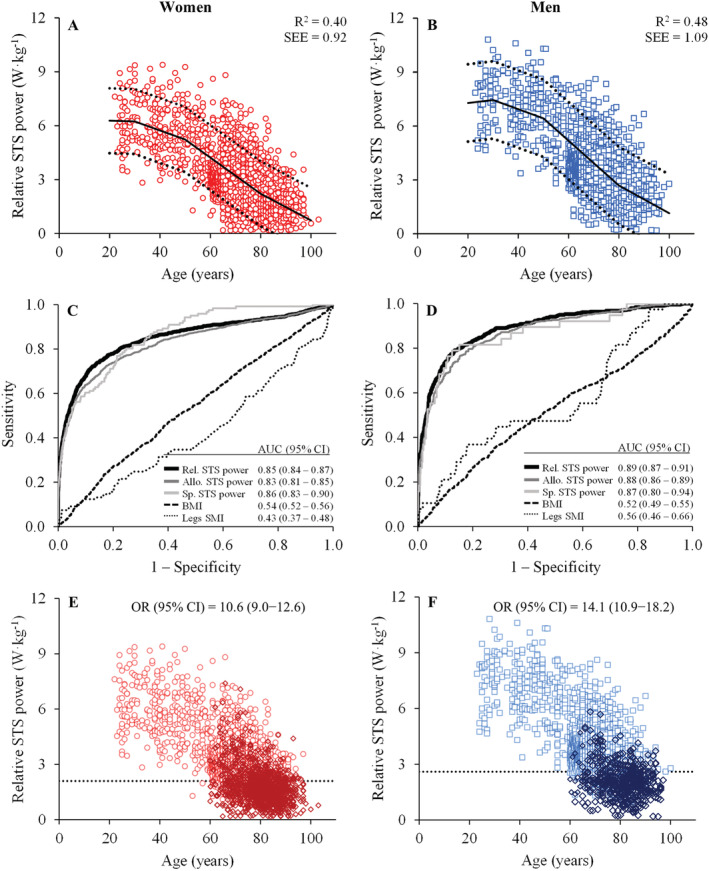
Relative STS power was found to decrease between 30-50 years (-0.05 W·kg ·year ; P > 0.05), 50-80 years (-0.10 to -0.13 W·kg ·year ; P < 0.001), and above 80 years (-0.07 to -0.08 W·kg ·year ; P < 0.001). A total of 1129 older women (18%) and 510 older men (16%) presented mobility limitations. Mobility-limited older adults were older and exhibited lower relative, allometric, and specific power; higher body mass index (BMI) and legs SMI (both only in women); and lower legs SMI (only in men) than their well-functioning counterparts (all P < 0.05). Normative data and cut-off points for relative, allometric, and specific STS power and for BMI and legs SMI were reported. Low relative STS power occurred below 2.1 W·kg in women (area under the curve, AUC, [95% confidence interval, CI] = 0.85 [0.84-0.87]) and below 2.6 W·kg in men (AUC [95% CI] = 0.89 [0.87-0.91]). The age-adjusted odds ratios [95% CI] for mobility limitations in older women and men with low relative STS power were 10.6 [9.0-12.6] and 14.1 [10.9-18.2], respectively. MCID values for relative STS power were 0.33 W·kg in women and 0.42 W·kg in men.
Relative STS power decreased significantly after the age of 50 years and was negatively and strongly associated with mobility limitations. Our study provides normative data, functionally relevant cut-off points, and MCID values for STS power for their use in daily clinical practice.
最近报道了一种经过验证、标准化且可行的评估老年人肌肉力量的测试:坐站(STS)肌肉力量测试。本研究旨在评估相对 STS 力量与年龄之间的关系,并为老年女性和男性的 STS 力量测量提供正常参考值、截断值和最小临床重要差异(MCID)。
共有 9320 名年龄在 60-103 岁的老年女性(6161 名)和老年男性(3159 名),以及 586 名年龄在 20-60 岁的年轻和中年成年人(318 名女性和 268 名男性)纳入本横断面研究。通过 30 秒 STS 力量测试评估相对(标准化为体重)、比例(标准化为身高平方)和特定(标准化为腿部肌肉质量)肌肉力量值。通过双能 X 射线吸收法和生物电阻抗分析法评估身体成分,计算腿部骨骼肌指数(标准化为身高平方)。收集习惯性和最大步行速度、计时起立行走测试和 6 分钟步行距离作为身体表现测量指标,并将参与者分为两组:功能良好和行动受限的老年人。
发现相对 STS 力量在 30-50 岁之间下降了 0.05W·kg·年(P>0.05),50-80 岁之间下降了 0.10 至 0.13W·kg·年(P<0.001),80 岁以上下降了 0.07 至 0.08W·kg·年(P<0.001)。共有 1129 名老年女性(18%)和 510 名老年男性(16%)表现出行动受限。行动受限的老年患者年龄更大,表现出相对较低的、比例和特定的力量;更高的体重指数(BMI)和腿部骨骼肌指数(仅女性);以及较低的腿部骨骼肌指数(仅男性)与功能良好的对照组(均 P<0.05)。报告了相对、比例和特定 STS 力量以及 BMI 和腿部骨骼肌指数的正常参考值和截断值。女性的相对 STS 力量低于 2.1W·kg(曲线下面积,AUC,[95%置信区间,CI]为 0.85 [0.84-0.87]),男性低于 2.6W·kg(AUC [95%CI]为 0.89 [0.87-0.91])时发生低相对 STS 力量。年龄调整后的优势比(95%CI)表明,女性和男性中相对 STS 力量低的老年人行动受限的风险分别为 10.6 [9.0-12.6]和 14.1 [10.9-18.2]。相对 STS 力量的 MCID 值为女性 0.33W·kg 和男性 0.42W·kg。
相对 STS 力量在 50 岁后显著下降,与行动受限呈负相关且高度相关。我们的研究为 STS 力量提供了正常参考值、功能相关的截断值和 MCID 值,可用于日常临床实践。