Møller Sidsel G, Rajan Shahzleen, Møller-Hansen Steen, Kragholm Kristian, Ringgren Kristian B, Folke Fredrik, Hansen Carolina Malta, Lippert Freddy K, Køber Lars, Gislason Gunnar, Torp-Pedersen Christian, Wissenberg Mads
Department of Cardiology, Copenhagen University Hospital Herlev and Gentofte, Hellerup, Denmark.
Unit of Epidemiology and Biostatistics, Aalborg University Hospital, Aalborg, Denmark.
Resusc Plus. 2020 Nov 4;4:100036. doi: 10.1016/j.resplu.2020.100036. eCollection 2020 Dec.
This study aimed to examine the impact of population density on bystander cardiopulmonary resuscitation (CPR) and survival after out-of-hospital cardiac arrest (OHCA).
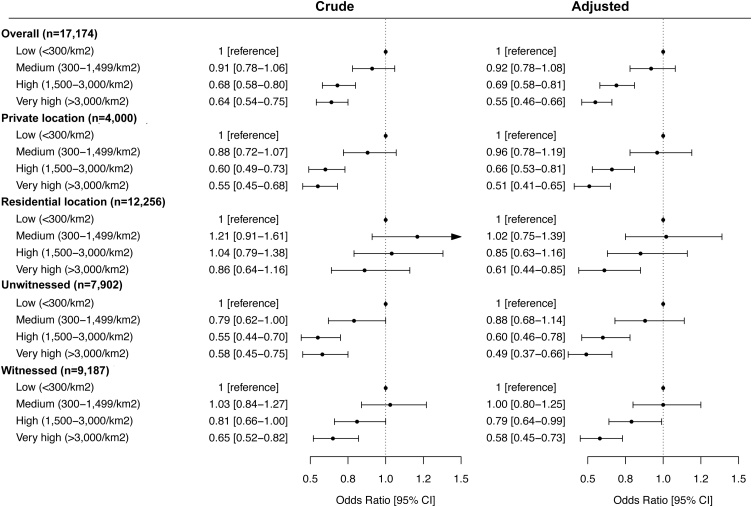
Through the Danish Cardiac Arrest Registry (2001-2013), OHCAs ≥18 years of presumed cardiac cause were identified, and divided according to the OHCA location in four population density groups (inhabitants/km) based on urban/rural area-definitions: low (<300/km), medium (300-1499/km), high (1500-2999/km), very high (>3000/km). The association between population density, bystander cardiopulmonary resuscitation (CPR) and survival was examined using logistic regression, adjusted for age, sex, comorbitidies and calendar-year.
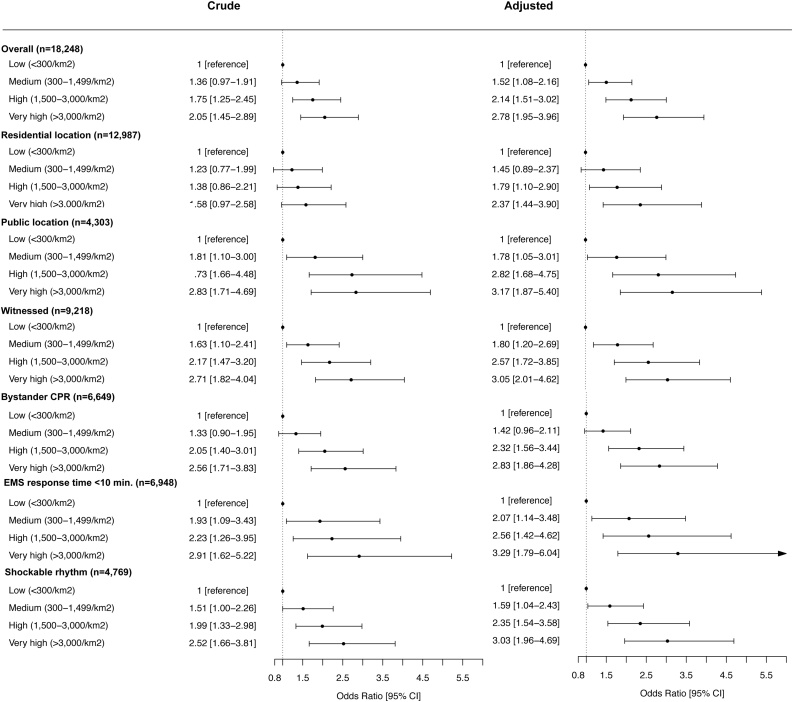
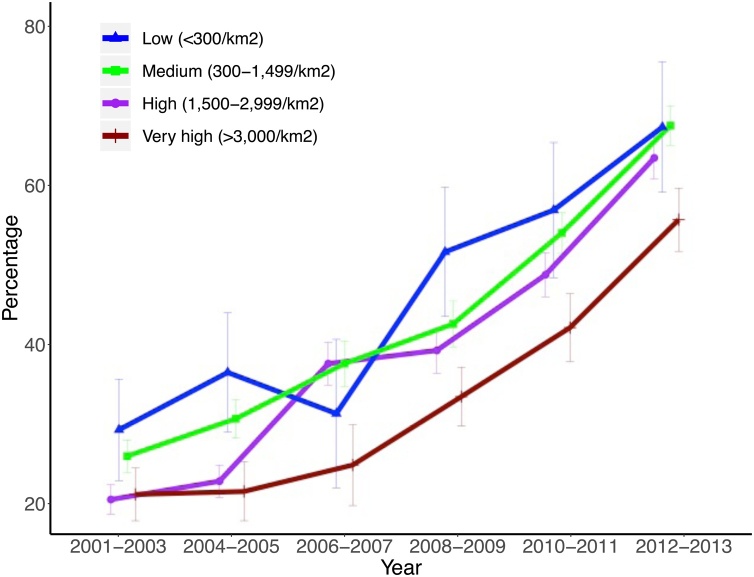
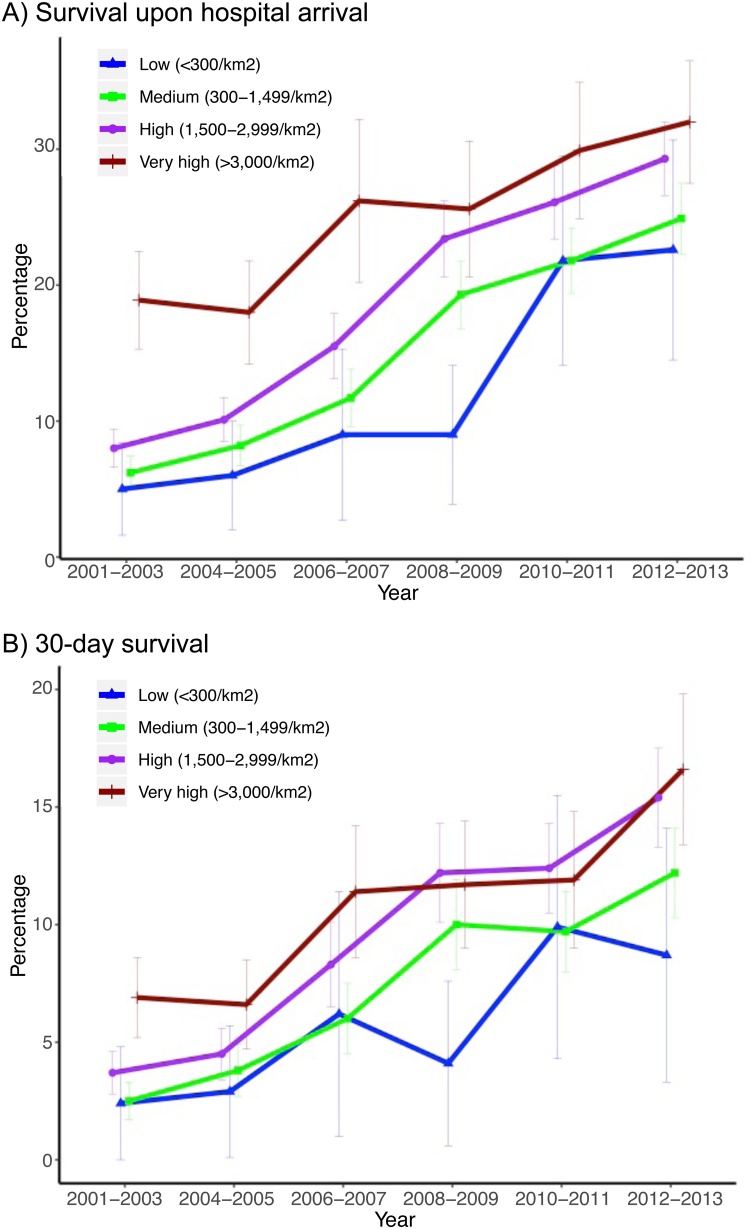
18,248 OHCAs were identified. Patients in areas of high compared to low population density were older, more often female, had more comorbidities, more witnessed arrests (very high: 59.6% versus low: 55.0%), shorter response time (very high: 10 min versus low: 14 min), but less bystander CPR (very high: 34.3% versus low: 45.1%). Thirty-day survival was higher in areas of higher population density (very high: 10.2% vs. low 5.3%), also in best-cases of witnessed arrests with bystander CPR and response time <10 min (very high: 33.6% versus low: 13.8%). The same trends were found in adjusted analyses with lower odds for bystander CPR (odds ratio [OR] 0.55 95% confidence interval [CI] 0.46-0.66) and higher odds for 30-day survival (OR 2.78, 95%CI 1.95-3.96) in the highest population density areas compared to low.
Having an OHCA in higher populated areas were found associated with less bystander CPR, but higher survival. Identification of area-related factors can help target future pre-hospital care.
本研究旨在探讨人口密度对院外心脏骤停(OHCA)后旁观者心肺复苏(CPR)及生存情况的影响。
通过丹麦心脏骤停登记处(2001 - 2013年),确定年龄≥18岁、推测病因是心脏原因的OHCA病例,并根据OHCA发生地点,依据城乡区域定义将其分为四个人口密度组(每平方公里居民数):低(<300/平方公里)、中(300 - 1499/平方公里)、高(1500 - 2999/平方公里)、非常高(>3000/平方公里)。采用逻辑回归分析人口密度、旁观者心肺复苏(CPR)与生存之间的关联,并对年龄、性别、合并症和历年情况进行校正。
共确定18248例OHCA病例。与低人口密度地区相比,高人口密度地区的患者年龄更大,女性更多,合并症更多,目击心脏骤停的情况更多(非常高:59.6% 对低:55.0%),反应时间更短(非常高:10分钟对低:14分钟),但旁观者进行心肺复苏的比例更低(非常高:34.3% 对低:45.1%)。高人口密度地区的30天生存率更高(非常高:10.2% 对低:5.3%),在目击心脏骤停且有旁观者进行心肺复苏且反应时间<10分钟的最佳情况下也是如此(非常高:33.6% 对低:13.8%)。在调整分析中发现了相同的趋势,与低人口密度地区相比,最高人口密度地区旁观者进行心肺复苏的几率更低(优势比[OR] 0.55,95%置信区间[CI] 0.46 - 0.66),30天生存的几率更高(OR 2.78,95%CI 1.95 - 3.96)。
发现在人口密度较高地区发生OHCA时,旁观者进行心肺复苏的情况较少,但生存率较高。识别与地区相关的因素有助于为未来的院前护理确定目标。