Ringgren Kristian Bundgaard, Kragholm Kristian Hay, Lindgren Filip Lyng, Jacobsen Peter Ascanius, Jørgensen Anne Juul, Christensen Helle Collatz, Mills Elisabeth Helen Anna, Jakobsen Louise Kollander, Yonis Harman, Folke Fredrik, Lippert Freddy, Torp-Pedersen Christian
Department of Cardiology, Aalborg University Hospital, Aalborg, Denmark.
Department of Respiratory Diseases, Aalborg University Hospital, Aalborg, Denmark.
Resusc Plus. 2022 Feb 1;9:100208. doi: 10.1016/j.resplu.2022.100208. eCollection 2022 Mar.
Geographical setting is seldomly taken into account when investigating out-of-hospital cardiac arrest (OHCA). It is a common notion that living in rural areas means a lower chance of fast and effective helpwhen suffering a time-critical event. This retrospective cohort study investigates this hypothesis and compares across healthcare-divided administrative regions.
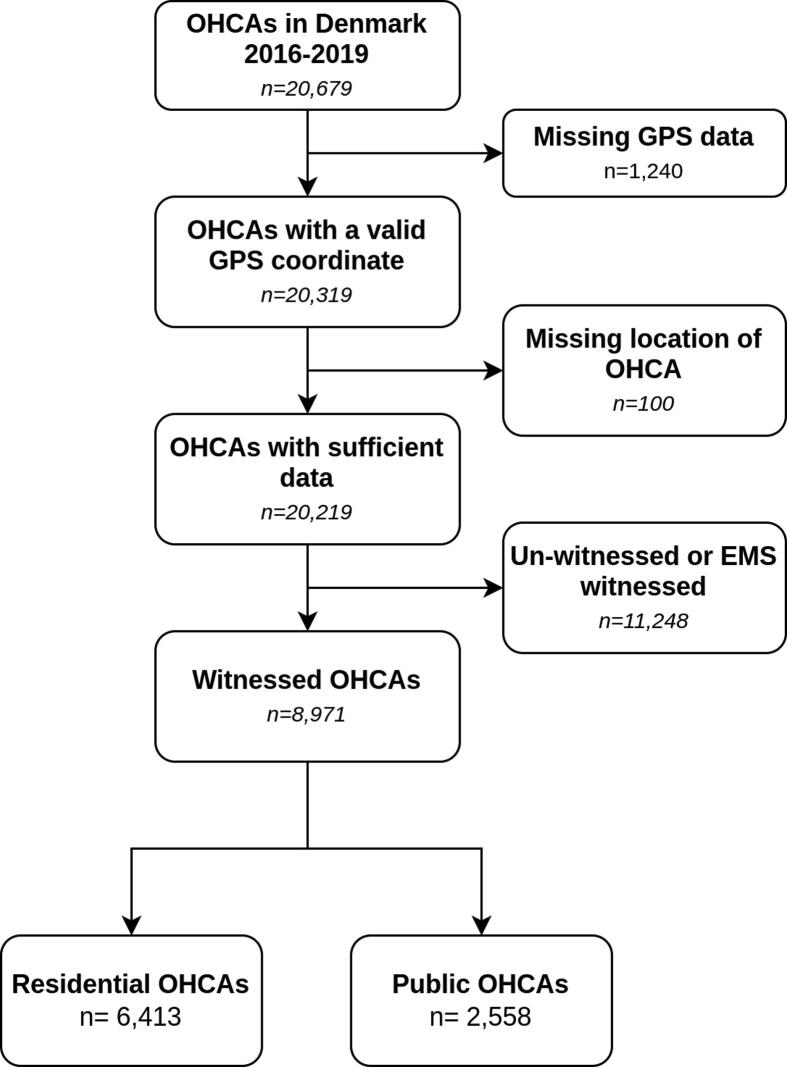
We included only witnessed OHCAs to minimize the risk that outcome was predetermined by time to caller arrival and/or recognition. Arrests were divided into public and residential. Residential arrests were categorized according to population density of the area in which they occurred. We investigated incidence, EMS response time and 30-day survival according to area type and subsidiarily by healthcare-divided administrative region.
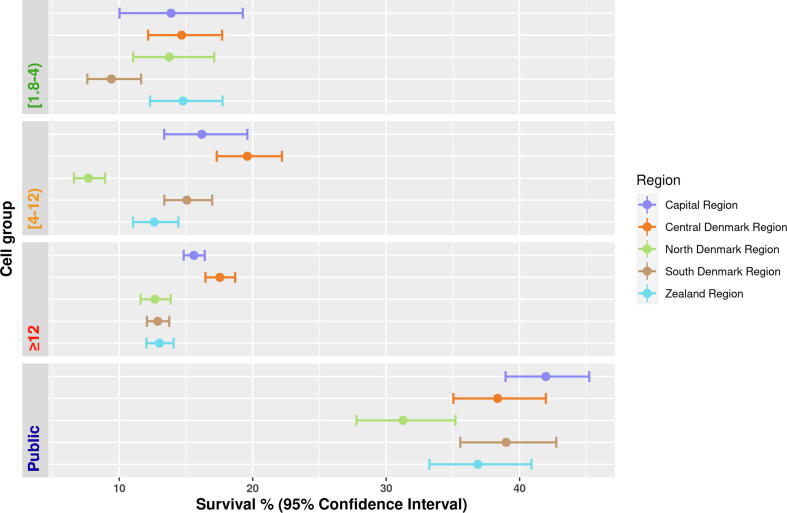
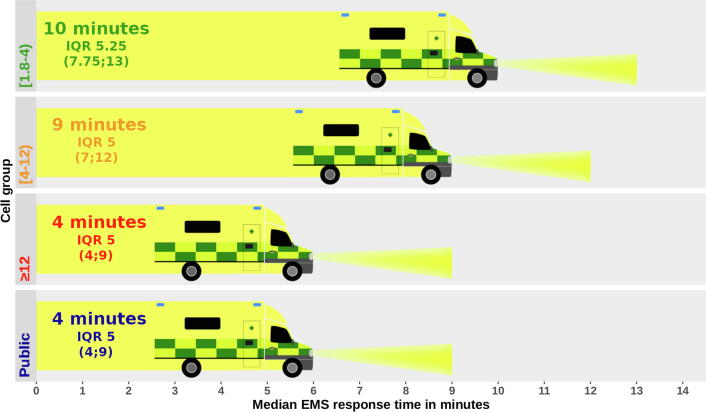
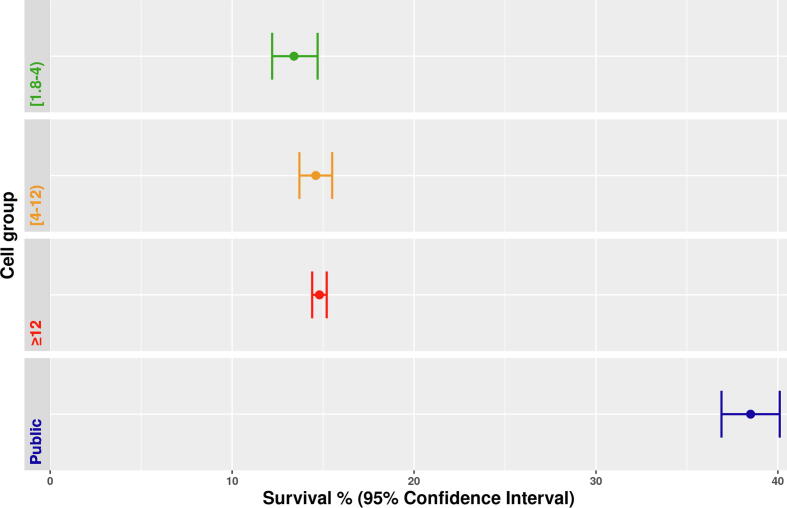
The majority (71%) of 8,579 OHCAs were residential, and 53.2% of all arrests occurred in the most densely populated cell group amongst residential arrests. This group had a median EMS response time of six minutes, whereas the most sparsely populated group had a median of 10 minutes. Public arrests also had a median response time of six minutes. 30-day survival was highest in public arrests (38.5%, [95% CI 36.9;40.1]), and varied only slightly with no statistical significance between OHCAs in densely and sparsely populated areas from 14.8% (95% CI 14.4;15.2) and 13.4% (95% CI 12.2;14.7).
Our study demonstrates that while EMS response times in Denmark are longer in the rural areas, there is no statistically significant decrease in survival compared to the most densely populated areas.
在调查院外心脏骤停(OHCA)时,很少考虑地理环境因素。人们普遍认为,生活在农村地区意味着在遭遇紧急情况时获得快速有效救助的机会较低。这项回顾性队列研究对这一假设进行了调查,并在不同医疗管理区域之间进行了比较。
我们仅纳入有目击者的院外心脏骤停病例,以尽量减少因呼叫者到达和/或识别时间而预先确定结果的风险。心脏骤停分为公共场所和住宅内两类。住宅内的心脏骤停根据发生地点的人口密度进行分类。我们根据区域类型并进一步按医疗管理区域调查了发病率、急救医疗服务(EMS)响应时间和30天生存率。
在8579例院外心脏骤停病例中,大多数(71%)发生在住宅内,所有心脏骤停病例中有53.2%发生在住宅内人口最密集的区域组。该组的急救医疗服务响应时间中位数为6分钟,而人口最稀少的组中位数为10分钟。公共场所心脏骤停的响应时间中位数也为6分钟。公共场所心脏骤停的30天生存率最高(38.5%,[95%置信区间36.9;40.1]),人口密集和稀少地区的院外心脏骤停病例的30天生存率仅略有差异,分别为14.8%(95%置信区间14.4;15.2)和13.4%(95%置信区间12.2;14.7),无统计学意义。
我们的研究表明,丹麦农村地区的急救医疗服务响应时间较长,但与人口最密集地区相比,生存率没有统计学上的显著下降。