Song Xiaoyu, Ji Jiayi, Reva Boris, Joshi Himanshu, Calinawan Anna Pamela, Mazumdar Madhu, Wisnivesky Juan P, Taioli Emanuela, Wang Pei, Veluswamy Rajwanth R
Institute for Healthcare Delivery Science, Dept of Population Health Science and Policy, Icahn School of Medicine at Mount Sinai, New York, NY, USA.
Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, NY, USA.
ERJ Open Res. 2021 Jul 5;7(3). doi: 10.1183/23120541.00018-2021. eCollection 2021 Jul.
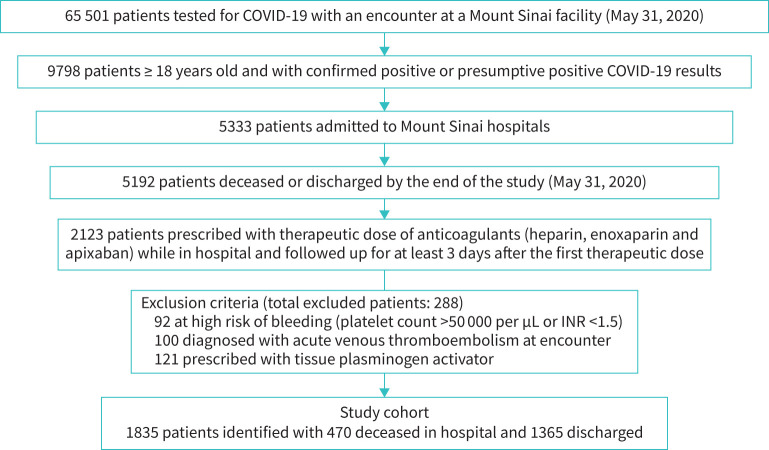
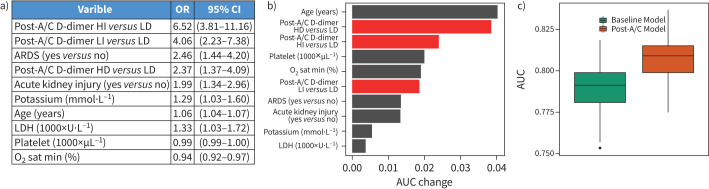
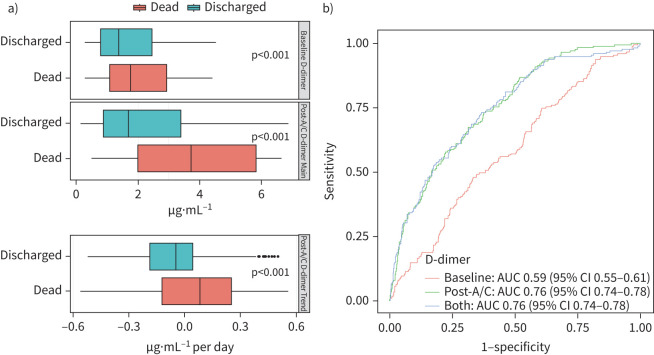
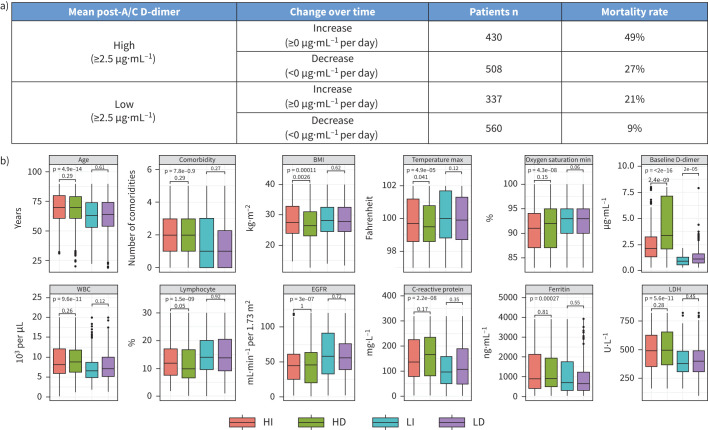
Clinical biomarkers that accurately predict mortality are needed for the effective management of patients with severe coronavirus disease 2019 (COVID-19) illness. In this study, we determine whether changes in D-dimer levels after anticoagulation are independently predictive of in-hospital mortality. Adult patients hospitalised for severe COVID-19 who received therapeutic anticoagulation for thromboprophylaxis were identified from a large COVID-19 database of the Mount Sinai Health System in New York City (NY, USA). We studied the ability of post-anticoagulant D-dimer levels to predict in-hospital mortality, while taking into consideration 65 other clinically important covariates including patient demographics, comorbidities, vital signs and several laboratory tests. 1835 adult patients with PCR-confirmed COVID-19 who received therapeutic anticoagulation during hospitalisation were included. Overall, 26% of patients died in the hospital. Significantly different in-hospital mortality rates were observed in patient groups based on mean D-dimer levels and trend following anticoagulation: 49% for the high mean-increase trend group; 27% for the high-decrease group; 21% for the low-increase group; and 9% for the low-decrease group (p<0.001). Using penalised logistic regression models to simultaneously analyse 67 clinical variables, the high increase (adjusted odds ratios (OR): 6.58, 95% CI 3.81-11.16), low increase (OR: 4.06, 95% CI 2.23-7.38) and high decrease (OR: 2.37; 95% CI 1.37-4.09) D-dimer groups (reference: low decrease group) had the highest odds for in-hospital mortality among all clinical features. Changes in D-dimer levels and trend following anticoagulation are highly predictive of in-hospital mortality and may help guide resource allocation and future studies of emerging treatments for severe COVID-19.
对于2019年冠状病毒病(COVID-19)重症患者的有效管理而言,需要能够准确预测死亡率的临床生物标志物。在本研究中,我们确定抗凝后D-二聚体水平的变化是否能独立预测住院死亡率。从美国纽约市西奈山医疗系统的一个大型COVID-19数据库中,识别出因重症COVID-19住院并接受预防性抗凝治疗的成年患者。我们研究了抗凝后D-二聚体水平预测住院死亡率的能力,同时考虑了65个其他临床重要协变量,包括患者人口统计学特征、合并症、生命体征和多项实验室检查。纳入了1835例住院期间接受治疗性抗凝的PCR确诊COVID-19成年患者。总体而言,26%的患者在医院死亡。根据抗凝后的平均D-二聚体水平和变化趋势,在患者组中观察到显著不同的住院死亡率:高平均升高趋势组为49%;高降低组为27%;低升高组为21%;低降低组为9%(p<0.001)。使用惩罚逻辑回归模型同时分析67个临床变量,高升高(调整后的比值比(OR):6.58,95%置信区间3.81-11.16)、低升高(OR:4.06,95%置信区间2.23-7.38)和高降低(OR:2.37;95%置信区间1.37-4.09)D-二聚体组(参照:低降低组)在所有临床特征中住院死亡率的几率最高。抗凝后D-二聚体水平的变化和趋势高度预测住院死亡率,可能有助于指导资源分配以及未来对重症COVID-19新疗法的研究。