Mbroh Joshua, Poli Khouloud, Tünnerhoff Johannes, Gomez-Exposito Alexandra, Wang Yi, Bender Benjamin, Hempel Johann-Martin, Hennersdorf Florian, Feil Katharina, Mengel Annerose, Ziemann Ulf, Poli Sven
Department of Neurology & Stroke, Eberhard-Karls University, Tübingen, Germany.
Hertie Institute for Clinical Brain Research, Eberhard-Karls University, Tübingen, Germany.
Front Neurol. 2021 Jun 22;12:687134. doi: 10.3389/fneur.2021.687134. eCollection 2021.
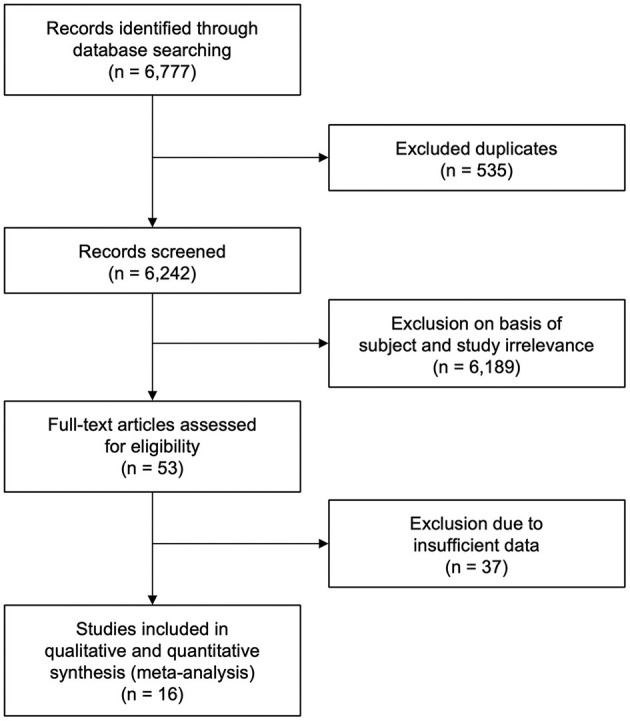
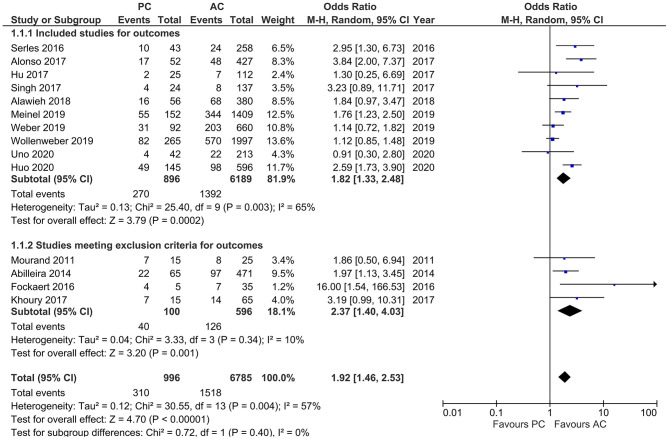
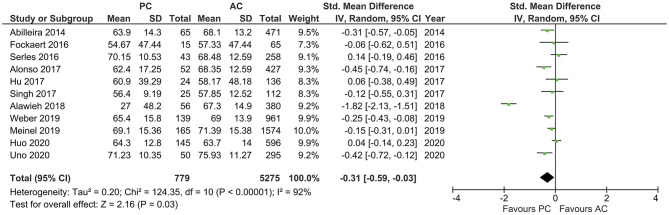
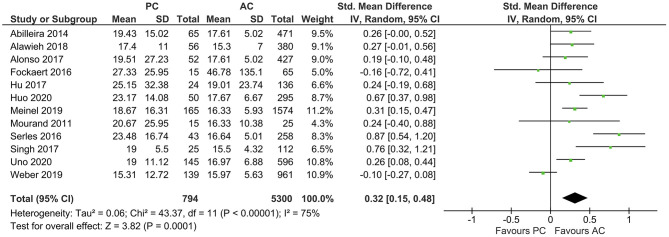
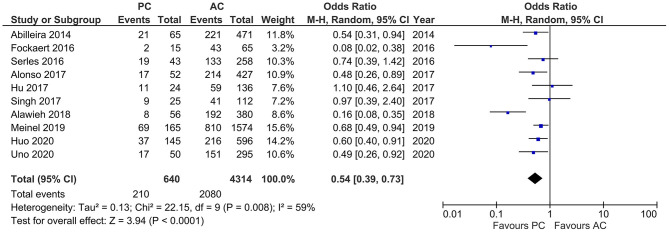
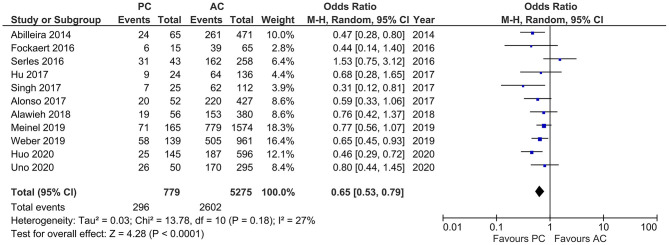
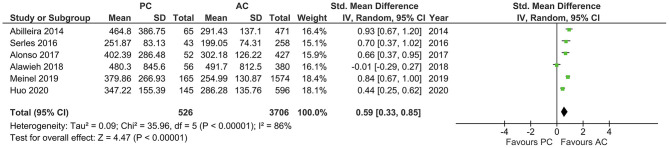
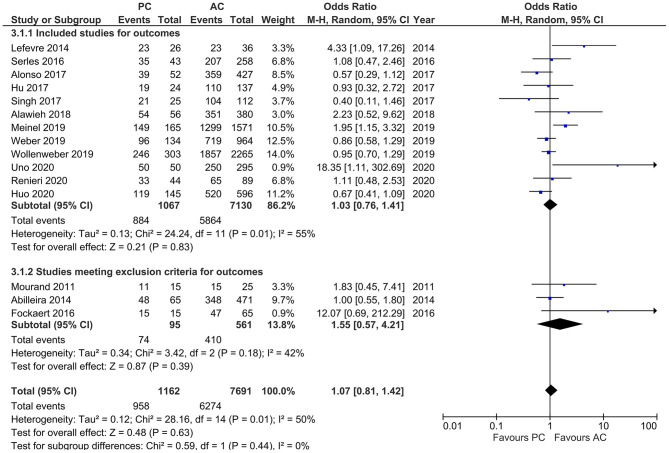
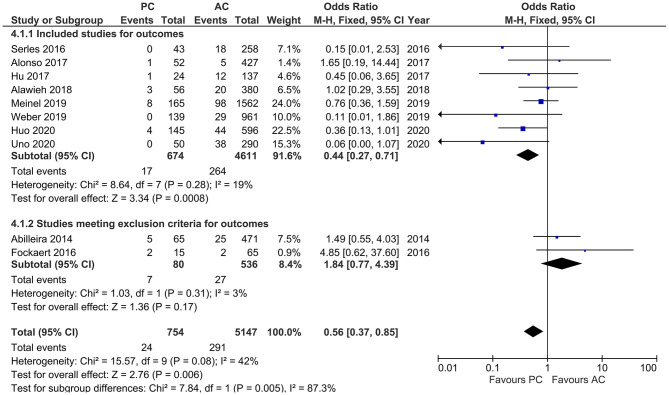
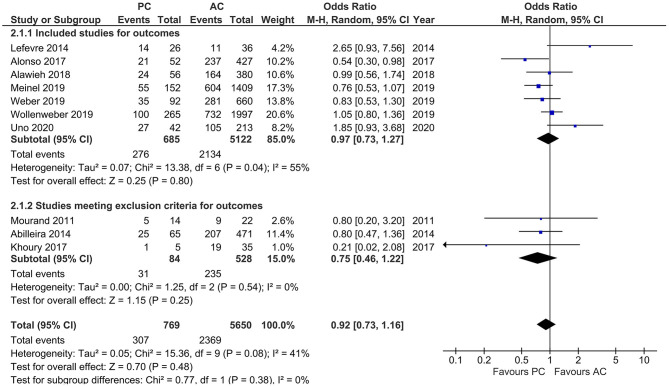
It is believed that stroke occurring due to posterior circulation large vessel occlusion (PCLVO) and that occurring due to anterior circulation large vessel occlusion (ACLVO) differ in terms of their pathophysiology and the outcome of their acute management in relation to endovascular mechanical thrombectomy (MT). Limited sample size and few randomized controlled trials (RCTs) with respect to PCLVO make the safety and efficacy of MT, which has been confirmed in ACLVO, difficult to assess in the posterior circulation. We therefore conducted a meta-analysis to study to which extent MT in PCLVO differs from ACLVO. We searched the databases PubMed, Cochrane, and EMBASE for studies published between 2010 and January 2021, with information on risk factors, safety, and efficacy outcomes of MT in PCLVO vs. ACLVO and conducted a systematic review and meta-analysis; we compared baseline characteristics, reperfusion treatment profiles [including rates of intravenous thrombolysis (IVT) and onset-to-IVT and onset-to-groin puncture times], recanalization success [Thrombolysis In Cerebral Infarction scale (TICI) 2b/3], symptomatic intracranial hemorrhage (sICH), and favorable functional outcome [modified Rankin Score (mRS) 0-2] and mortality at 90 days. Sixteen studies with MT PCLVO (1,172 patients) and ACLVO (7,726 patients) were obtained from the search. The pooled estimates showed higher baseline National Institutes of Health Stroke Scale (NIHSS) score (SMD 0.32, 95% CI 0.15-0.48) in the PCLVO group. PCLVO patients received less often IVT (OR 0.65, 95% CI 0.53-0.79). Onset-to-IVT time (SMD 0.86, 95% CI 0.45-1.26) and onset-to-groin puncture time (SMD 0.59, 95% CI 0.33-0.85) were longer in the PCLVO group. The likelihood of obtaining successful recanalization and favorable functional outcome at 90 days was comparable between the two groups. PCLVO was, however, associated with less sICH (OR 0.56, 95% CI 0.37-0.85) but higher mortality (OR 1.92, 95% CI 1.46-2.53). This meta-analysis indicates that MT in PCLVO may be comparably efficient in obtaining successful recanalization and 90 day favorable functional outcome just as in ACLVO. Less sICH in MT-treated PCLVO patients might be the result of the lower IVT rate in this group. Higher baseline NIHSS and longer onset-to-IVT and onset-to-groin puncture times may have contributed to a higher 90 day mortality in PCLVO patients.
据信,由后循环大血管闭塞(PCLVO)导致的中风与由前循环大血管闭塞(ACLVO)导致的中风在病理生理学以及与血管内机械取栓术(MT)相关的急性治疗结果方面存在差异。关于PCLVO的样本量有限且随机对照试验(RCT)较少,这使得已在ACLVO中得到证实的MT的安全性和有效性在后循环中难以评估。因此,我们进行了一项荟萃分析,以研究PCLVO中的MT与ACLVO中的MT在何种程度上存在差异。我们在PubMed、Cochrane和EMBASE数据库中搜索了2010年至2021年1月发表的研究,这些研究包含PCLVO与ACLVO中MT的危险因素、安全性和有效性结果的信息,并进行了系统评价和荟萃分析;我们比较了基线特征、再灌注治疗情况[包括静脉溶栓(IVT)率以及发病至IVT和发病至腹股沟穿刺时间]、再通成功情况[脑梗死溶栓量表(TICI)2b/3]、有症状颅内出血(sICH)、良好功能结局[改良Rankin量表(mRS)0 - 2]以及90天死亡率。通过搜索获得了16项关于MT治疗PCLVO(1172例患者)和ACLVO(7726例患者)的研究。汇总估计显示,PCLVO组的基线美国国立卫生研究院卒中量表(NIHSS)评分更高(标准化均值差0.32,95%置信区间0.15 - 0.48)。PCLVO患者接受IVT的频率较低(比值比0.65,95%置信区间0.53 - 0.79)。PCLVO组的发病至IVT时间(标准化均值差0.86,95%置信区间0.45 - 1.26)和发病至腹股沟穿刺时间(标准化均值差0.59,95%置信区间0.33 - 0.85)更长。两组在90天时获得成功再通和良好功能结局的可能性相当。然而,PCLVO与较少的sICH相关(比值比0.56,95%置信区间0.37 - 0.85),但死亡率较高(比值比1.92,95%置信区间1.46 - 2.53)。这项荟萃分析表明,PCLVO中的MT在获得成功再通和90天良好功能结局方面可能与ACLVO中的MT同样有效。MT治疗的PCLVO患者中sICH较少可能是该组IVT率较低的结果。较高的基线NIHSS以及较长的发病至IVT和发病至腹股沟穿刺时间可能导致PCLVO患者90天死亡率较高。