2nd Department of General Surgery, Jagiellonian University Medical College, Jakubowskiego 2 st., 30-688, Kraków, Poland.
Department of General Surgery and Surgical Oncology, Ludwik Rydygier Memorial Hospital in Cracow, Kraków, Poland.
Langenbecks Arch Surg. 2022 Feb;407(1):131-141. doi: 10.1007/s00423-021-02260-3. Epub 2021 Jul 13.
Bariatric surgery has proven to be the most efficient treatment for obesity and type 2 diabetes mellitus (T2DM). Despite detailed qualification, desirable outcome after an intervention is not achieved by every patient. Various risk prediction models of diabetes remission after metabolic surgery have been established to facilitate the decision-making process. The purpose of the study is to validate the performance of available risk prediction scores for diabetes remission a year after surgical treatment and to determine the optimal model.
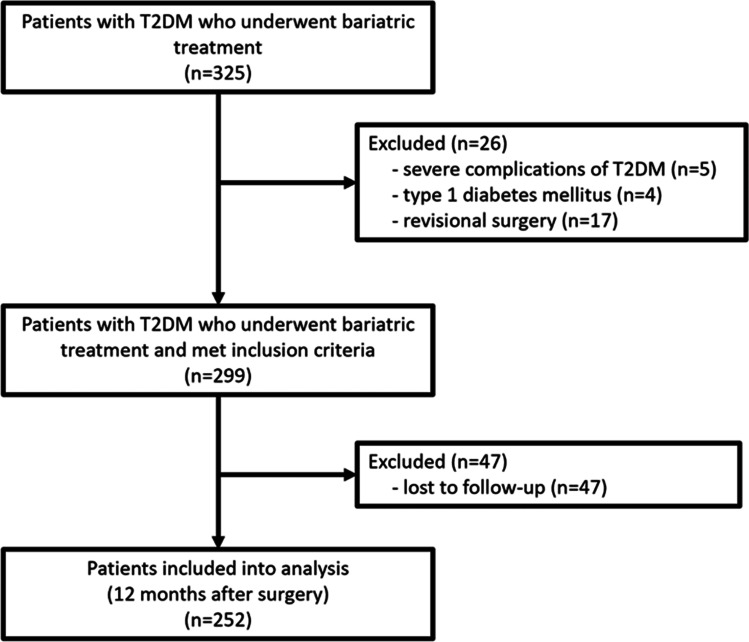
A retrospective analysis comprised 252 patients who underwent Roux-en-Y gastric bypass (RYGB) or sleeve gastrectomy (SG) between 2009 and 2017 and completed 1-year follow-up. The literature review revealed 5 models, which were subsequently explored in our study. Each score relationship with diabetes remission was assessed using logistic regression. Discrimination was evaluated by area under the receiver operating characteristic (AUROC) curve, whereas calibration by the Hosmer-Lemeshow test and predicted versus observed remission ratio.
One year after surgery, 68.7% partial and 21.8% complete diabetes remission and 53.4% excessive weight loss were observed. DiaBetter demonstrated the best predictive performance (AUROC 0.81; 95% confidence interval (CI) 0.71-0.90; p-value > 0.05 in the Hosmer-Lemeshow test; predicted-to-observed ratio 1.09). The majority of models showed acceptable discrimination power. In calibration, only the DiaBetter score did not lose goodness-of-fit in all analyzed groups.
The DiaBetter score seems to be the most appropriate tool to predict diabetes remission after metabolic surgery since it presents adequate accuracy and is convenient to use in clinical practice. There are no accurate models to predict T2DM remission in a patient with advanced diabetes.
减重手术已被证明是治疗肥胖症和 2 型糖尿病(T2DM)最有效的方法。尽管进行了详细的资格评估,但并非每个患者都能达到理想的干预效果。已经建立了各种代谢手术后糖尿病缓解的风险预测模型,以促进决策过程。本研究的目的是验证现有糖尿病缓解风险预测评分在手术后 1 年的性能,并确定最佳模型。
回顾性分析了 2009 年至 2017 年间接受 Roux-en-Y 胃旁路术(RYGB)或袖状胃切除术(SG)治疗并完成 1 年随访的 252 例患者。文献复习显示了 5 种模型,随后在我们的研究中进行了探讨。使用逻辑回归评估每个评分与糖尿病缓解的关系。通过接受者操作特征(ROC)曲线下面积(AUROC)评估区分度,通过 Hosmer-Lemeshow 检验和预测与观察缓解比评估校准度。
术后 1 年,部分缓解 68.7%,完全缓解 21.8%,体重减轻过多 53.4%。DiaBetter 表现出最佳的预测性能(AUROC 0.81;95%置信区间 [CI] 0.71-0.90;Hosmer-Lemeshow 检验 p 值>0.05;预测与观察比值 1.09)。大多数模型的区分能力都可以接受。在校准方面,只有 DiaBetter 评分在所有分析组中都没有失去拟合优度。
由于 DiaBetter 评分具有足够的准确性,并且在临床实践中使用方便,因此它似乎是预测代谢手术后糖尿病缓解的最恰当工具。对于患有晚期糖尿病的患者,目前还没有准确的模型可以预测 T2DM 的缓解。