Howes Oliver D, Thase Michael E, Pillinger Toby
Institute of Psychiatry, Psychology and Neuroscience, King's College London, London, UK.
MRC London Institute of Medical Sciences, Faculty of Medicine, Imperial College London, Hammersmith Hospital Campus, London, UK.
Mol Psychiatry. 2022 Jan;27(1):58-72. doi: 10.1038/s41380-021-01200-3. Epub 2021 Jul 13.
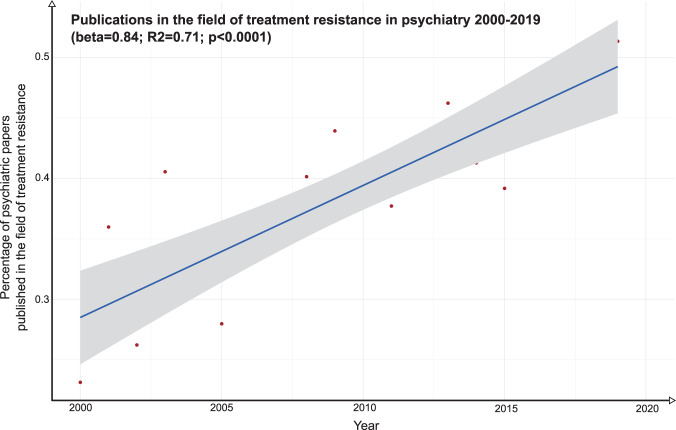
Treatment resistance affects 20-60% of patients with psychiatric disorders; and is associated with increased healthcare burden and costs up to ten-fold higher relative to patients in general. Whilst there has been a recent increase in the proportion of psychiatric research focussing on treatment resistance (R = 0.71, p < 0.0001), in absolute terms this is less than 1% of the total output and grossly out of proportion to its prevalence and impact. Here, we provide an overview of treatment resistance, considering its conceptualisation, assessment, epidemiology, impact, and common neurobiological models. We also review new treatments in development and future directions. We identify 23 consensus guidelines on its definition, covering schizophrenia, major depressive disorder, bipolar affective disorder, and obsessive compulsive disorder (OCD). This shows three core components to its definition, but also identifies heterogeneity and lack of criteria for a number of disorders, including panic disorder, post-traumatic stress disorder, and substance dependence. We provide a reporting check-list to aid comparisons across studies. We consider the concept of pseudo-resistance, linked to poor adherence or other factors, and provide an algorithm for the clinical assessment of treatment resistance. We identify nine drugs and a number of non-pharmacological approaches being developed for treatment resistance across schizophrenia, major depressive disorder, bipolar affective disorder, and OCD. Key outstanding issues for treatment resistance include heterogeneity and absence of consensus criteria, poor understanding of neurobiology, under-investment, and lack of treatments. We make recommendations to address these issues, including harmonisation of definitions, and research into the mechanisms and novel interventions to enable targeted and personalised therapeutic approaches.
治疗抵抗影响20%至60%的精神疾病患者;并与医疗负担增加和成本上升相关,相对于普通患者,成本高出多达十倍。尽管最近专注于治疗抵抗的精神科研究比例有所增加(R = 0.71,p < 0.0001),但从绝对数量来看,这不到总产出的1%,与其患病率和影响严重不成比例。在此,我们概述治疗抵抗,考虑其概念化、评估、流行病学、影响和常见的神经生物学模型。我们还回顾了正在研发的新治疗方法和未来方向。我们确定了23条关于其定义的共识指南,涵盖精神分裂症、重度抑郁症、双相情感障碍和强迫症(OCD)。这显示了其定义的三个核心组成部分,但也指出了包括惊恐障碍、创伤后应激障碍和物质依赖在内的一些疾病存在异质性且缺乏标准。我们提供了一个报告清单,以帮助进行跨研究比较。我们考虑了与依从性差或其他因素相关的假性抵抗概念,并提供了一种治疗抵抗临床评估算法。我们确定了九种正在针对精神分裂症、重度抑郁症、双相情感障碍和强迫症的治疗抵抗进行研发的药物以及一些非药物方法。治疗抵抗的关键突出问题包括异质性和缺乏共识标准、对神经生物学理解不足、投资不足以及缺乏治疗方法。我们提出了解决这些问题的建议,包括统一定义,以及对机制和新型干预措施进行研究,以实现有针对性的个性化治疗方法。