From the Cardiology Department, Mother and Child Health Institute of Serbia.
School of Medicine, University of Belgrade.
Pediatr Infect Dis J. 2021 Nov 1;40(11):e390-e394. doi: 10.1097/INF.0000000000003260.
Cardiovascular complications with myocarditis in multisystem inflammatory syndrome in children (MIS-C) associated with severe acute respiratory syndrome coronavirus 2 infection have been reported, but the optimal therapeutic strategy remains unknown.
A retrospective cohort study included 19 patients with acute left ventricular systolic dysfunction associated with MIS-C, average years of age 13.2 ± 3.8, treated from April 2020 to April 2021.
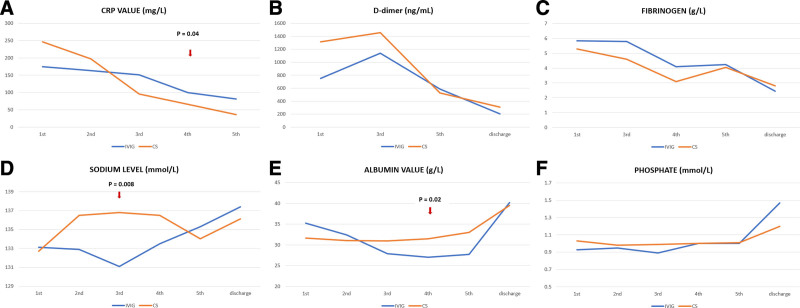
Treatment failure (TF) was observed in 8 patients (in the intravenous immunoglobulin [IVIG] group 7/10; in the corticosteroid [CS] group 1/9). The independent risk factor for TF was IVIG treatment (odds ratio [OR] 18.6, 95% confidence interval [CI] 1.6-222.93, P = 0.02). Patients initially treated with CS became afebrile during in-hospital day 1 (1.5, interquartile range [IQR] 1-2), while IVIG-treated patients became afebrile on in-hospital day 4 (IQR 2-4.25), after CS was added. The C-reactive protein (CRP) significantly declined in CS-treated patients on day 2 (P = 0.01), while in the IVIG group, CRP decreased significantly on the fourth day (P = 0.04). Sodium and albumin levels were higher on third in-hospital day in the CS group than in the IVIG group (P = 0.015, P = 0.03). A significant improvement and normalization of ejection fraction (EF) during the first 3 days was observed only in the CS group (P = 0.005). ICU stays were shorter in the CS group (4, IQR 2-5.5) than in the IVIG group (IVIG group 7, IQR 6-8.5) (P = 0.002).
Among children with MIS-C with cardiovascular involvement, treatment with CS was associated with faster normalization of LV EF, fever, laboratory analysis, and shorter ICU than IVIG-treated patients.
与严重急性呼吸综合征冠状病毒 2 感染相关的儿童多系统炎症综合征 (MIS-C) 并发心肌炎可导致心血管并发症,但最佳治疗策略仍不清楚。
本回顾性队列研究纳入了 19 例急性左心室收缩功能障碍合并 MIS-C 的患者,平均年龄为 13.2±3.8 岁,治疗时间为 2020 年 4 月至 2021 年 4 月。
观察到 8 例患者(静脉注射免疫球蛋白 [IVIG] 组 7/10 例;皮质类固醇 [CS] 组 1/9 例)治疗失败 (TF)。TF 的独立危险因素是 IVIG 治疗(比值比 [OR] 18.6,95%置信区间 [CI] 1.6-222.93,P=0.02)。最初接受 CS 治疗的患者在住院第 1 天(1.5,四分位距 [IQR] 1-2)时退热,而接受 IVIG 治疗的患者在 CS 加用时在住院第 4 天(IQR 2-4.25)退热。CS 治疗组患者的 C 反应蛋白 (CRP) 在第 2 天显著下降(P=0.01),而在 IVIG 组,CRP 在第 4 天显著下降(P=0.04)。CS 组患者在住院第 3 天的血清钠和白蛋白水平高于 IVIG 组(P=0.015,P=0.03)。仅在 CS 组观察到 EF 在最初 3 天内显著改善和正常化(P=0.005)。CS 组患者的 ICU 住院时间短于 IVIG 组(CS 组 4,IQR 2-5.5;IVIG 组 7,IQR 6-8.5)(P=0.002)。
在合并心血管受累的 MIS-C 患儿中,与 IVIG 治疗相比,CS 治疗可更快地使左心室射血分数 (EF) 正常化,退热,改善实验室分析,并缩短 ICU 住院时间。