Vella Laura A, Rowley Anne H
Division of Infectious Diseases, Department of Pediatrics, Children's Hospital of Philadelphia, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA 19104 USA.
Institute for Immunology, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA 19104 USA.
Curr Pediatr Rep. 2021;9(4):83-92. doi: 10.1007/s40124-021-00257-6. Epub 2021 Oct 19.
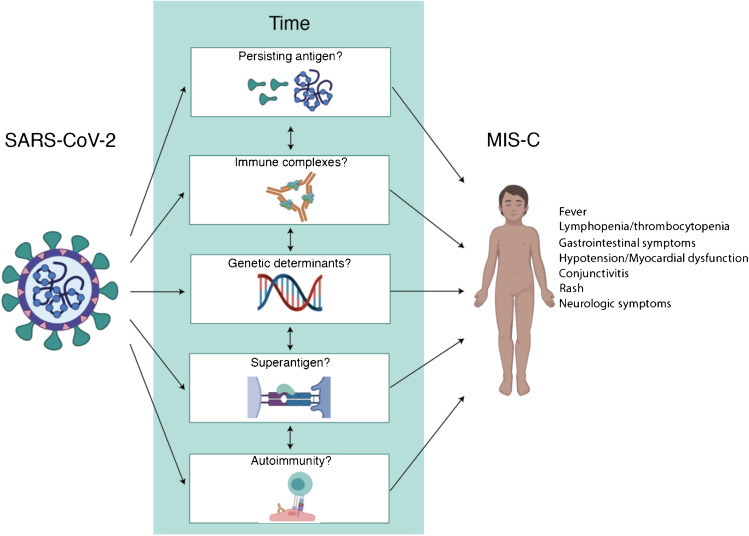
We highlight the new clinical entity multisystem inflammatory syndrome in children (MIS-C), the progress in understanding its immunopathogenesis, and compare and contrast the clinical and immunologic features of MIS-C with Kawasaki disease (KD).
Studies show immune dysregulation in MIS-C including T lymphocyte depletion and activation, T cell receptor Vbeta skewing, elevated plasmablast frequencies, increased markers of vascular pathology, and decreased numbers and functional profiles of antigen-presenting cells.
MIS-C is a late manifestation of infection with SARS-CoV-2 associated with marked immune activation and many potential mechanisms of immunopathogenesis. MIS-C and KD have clinical similarities but are distinct. Myocardial dysfunction with or without mild coronary artery dilation can occur in MIS-C but generally corrects within weeks. In contrast, the coronary arteries are the primary target in KD, and coronary artery sequelae can be lifelong. Supportive care and anti-inflammatory therapy appear to hasten improvement in children with MIS-C, and there is hope that vaccines will prevent its development.
我们重点介绍儿童多系统炎症综合征(MIS-C)这一新的临床实体,阐述在理解其免疫发病机制方面取得的进展,并比较和对比MIS-C与川崎病(KD)的临床和免疫学特征。
研究显示MIS-C存在免疫失调,包括T淋巴细胞耗竭与活化、T细胞受体Vβ偏移、浆母细胞频率升高、血管病理标志物增加以及抗原呈递细胞数量和功能谱降低。
MIS-C是严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染的晚期表现,与显著的免疫激活及多种免疫发病机制相关。MIS-C与KD有临床相似性,但又有所不同。MIS-C可出现伴或不伴轻度冠状动脉扩张的心肌功能障碍,但通常在数周内恢复正常。相比之下,冠状动脉是KD的主要靶器官,冠状动脉后遗症可能会伴随终生。支持性治疗和抗炎治疗似乎能加速MIS-C患儿的病情改善,并且有望通过疫苗预防其发生。