Carter G, Govindan R B, Brown G, Heimann C, Hayes H, Thostenson J C, Dornhoffer J, Brozoski T, Kimbrell T A, Hayar A, Shihabuddin B, James G A, Garcia-Rill E, Padala P R, Mennemeier M
Department of Anatomy and Physiology, National Park College, USA.
Prenatal Pediatrics Institute, Children's National Hospital, USA.
Front Neurol Neurosci Res. 2021;2. Epub 2021 May 17.
To examine how 1Hz and 10Hz rTMS temporarily influence ratings of tinnitus loudness, annoyance, and awareness. The thalamocortical dysrhythmia (TCD) model of tinnitus was tested by examining changes in spectral power and coherence of resting state EEGs from baseline to each phase of treatment and correlating these data with change in tinnitus.
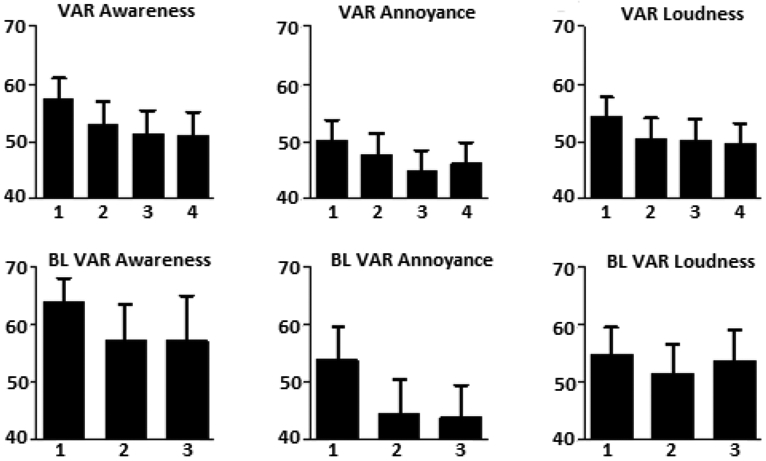
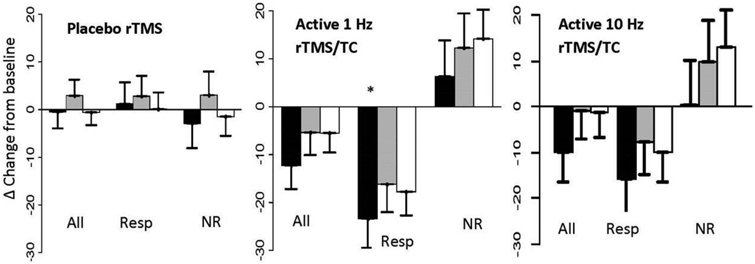
Nineteen participants completed a double-blind, placebo (sham rTMS) controlled, within-subjects study with crossover between the two active rTMS treatment conditions. An imposed order effect, sham rTMS first, eliminated drift of active treatment into the placebo condition. The primary outcome measures were analogue ratings of tinnitus loudness, annoyance, and awareness, assessed repeatedly at baseline and during treatment, and 64 channel, resting state EEGs collected at baseline and the end of each treatment phase. Active rTMS consisted of 1800 pulses at 110% of motor threshold over temporal cortex delivered at 1Hz and 10Hz over four days. The research design also examined the effect of rTMS immediately following stimulation, regression to the mean in tinnitus ratings made over multiple days, and differences between treatment responders and non-responders.
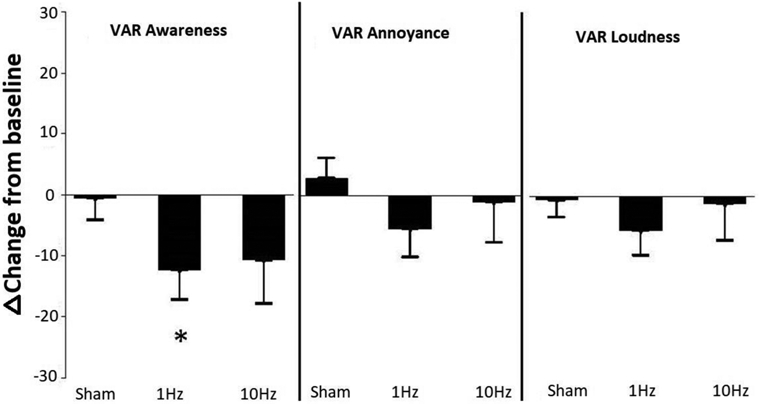
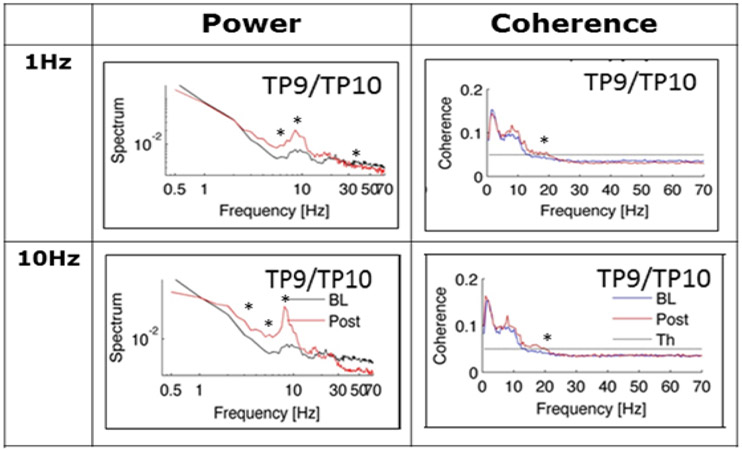
There was no immediate effect of rTMS on tinnitus during a single rTMS session. Regression to the mean in tinnitus ratings occurred over three days of baseline and four days of treatment (both sham and active rTMS). After accounting for regression to the mean in the statistical model, 1Hz rTMS led to a significant decrease in tinnitus awareness from baseline and 10Hz rTMS trended in the same direction, whereas sham rTMS showed little change from baseline other than regression to the mean. Changes from baseline in spectral power of the resting state EEG provided partial support for predictions based on TCD model of tinnitus for active 1 and 10Hz rTMS but not sham rTMS. However, only an increase in beta coherence correlated significantly with a decrease in tinnitus awareness. Changes in the EEG were robust in treatment responders but absent among non-responders and during sham rTMS.
A positive response to rTMS for tinnitus is associated with an rTMS-induced change in beta coherence of the EEG. Increased beta coherence may be a biomarker of the rTMS effect; a "top-down" modulation of the EEG that promotes habituation to tinnitus. Participants whose tinnitus did not improve after rTMS did not show any changes in the EEG.
研究1Hz和10Hz重复经颅磁刺激(rTMS)如何暂时影响耳鸣响度、烦恼程度及知晓度的评分。通过检查静息态脑电图从基线到治疗各阶段的频谱功率和相干性变化,并将这些数据与耳鸣变化相关联,对耳鸣的丘脑皮质节律紊乱(TCD)模型进行测试。
19名参与者完成了一项双盲、安慰剂(假rTMS)对照的受试者内研究,在两种活性rTMS治疗条件之间进行交叉。采用假rTMS先进行的强制顺序效应,消除活性治疗向安慰剂条件的漂移。主要结局指标为耳鸣响度、烦恼程度及知晓度的模拟评分,在基线和治疗期间重复评估,以及在基线和每个治疗阶段结束时收集的64通道静息态脑电图。活性rTMS包括在颞叶皮质运动阈值的110%下,以1Hz和10Hz分别给予1800个脉冲,持续四天。研究设计还检查了刺激后立即进行的rTMS的效果、多天耳鸣评分的均值回归,以及治疗反应者和无反应者之间的差异。
单次rTMS治疗期间,rTMS对耳鸣无即时效应。耳鸣评分在基线三天和治疗四天(假rTMS和活性rTMS)期间出现均值回归。在统计模型中考虑均值回归后,1Hz rTMS导致耳鸣知晓度较基线显著降低,10Hz rTMS也呈相同趋势,而假rTMS除均值回归外,与基线相比变化不大。静息态脑电图频谱功率相对于基线的变化为基于耳鸣TCD模型对活性1Hz和10Hz rTMS的预测提供了部分支持,但对假rTMS不适用。然而,只有β波相干性增加与耳鸣知晓度降低显著相关。脑电图变化在治疗反应者中明显,但在无反应者和假rTMS期间未出现。
对耳鸣的rTMS阳性反应与rTMS诱导的脑电图β波相干性变化相关。β波相干性增加可能是rTMS效应的生物标志物;一种促进对耳鸣习惯化的脑电图“自上而下”调制。rTMS后耳鸣未改善的参与者脑电图未显示任何变化。