Lancet. 2021 Jul 24;398(10297):325-339. doi: 10.1016/S0140-6736(21)00767-4. Epub 2021 Jul 13.
Congenital anomalies are the fifth leading cause of mortality in children younger than 5 years globally. Many gastrointestinal congenital anomalies are fatal without timely access to neonatal surgical care, but few studies have been done on these conditions in low-income and middle-income countries (LMICs). We compared outcomes of the seven most common gastrointestinal congenital anomalies in low-income, middle-income, and high-income countries globally, and identified factors associated with mortality.
We did a multicentre, international prospective cohort study of patients younger than 16 years, presenting to hospital for the first time with oesophageal atresia, congenital diaphragmatic hernia, intestinal atresia, gastroschisis, exomphalos, anorectal malformation, and Hirschsprung's disease. Recruitment was of consecutive patients for a minimum of 1 month between October, 2018, and April, 2019. We collected data on patient demographics, clinical status, interventions, and outcomes using the REDCap platform. Patients were followed up for 30 days after primary intervention, or 30 days after admission if they did not receive an intervention. The primary outcome was all-cause, in-hospital mortality for all conditions combined and each condition individually, stratified by country income status. We did a complete case analysis.
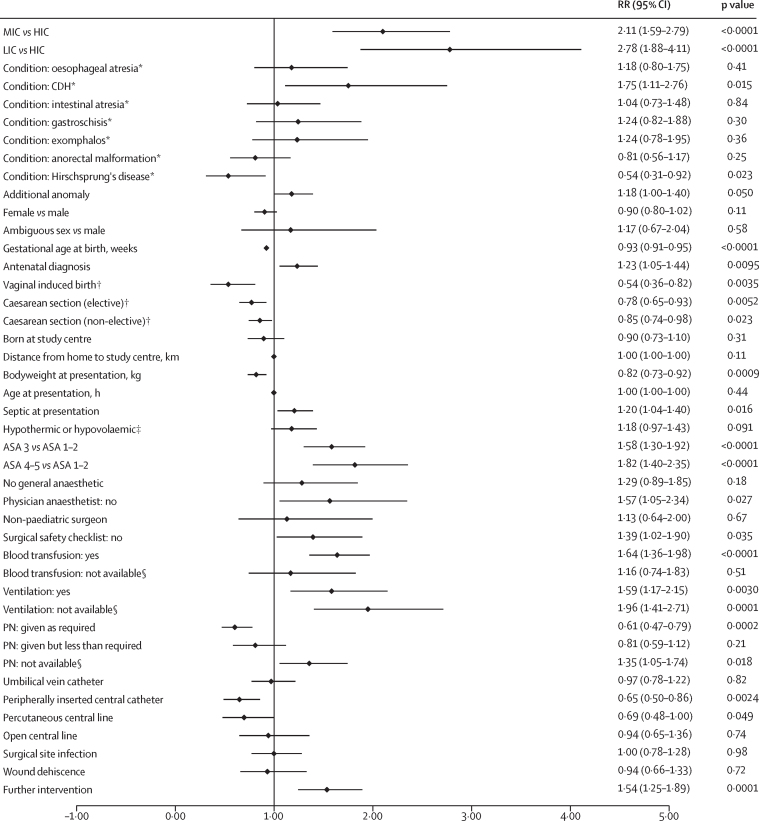
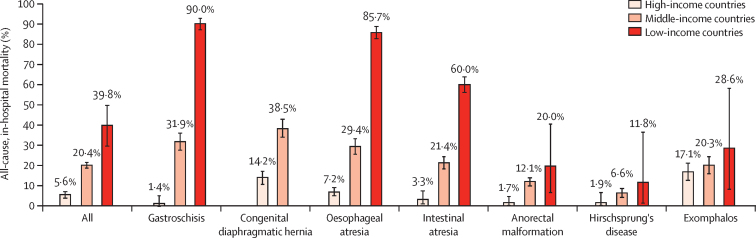
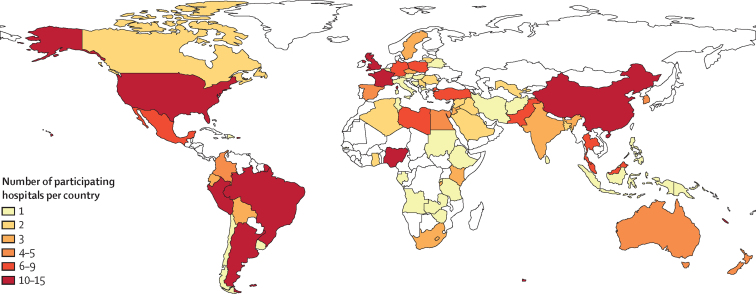
We included 3849 patients with 3975 study conditions (560 with oesophageal atresia, 448 with congenital diaphragmatic hernia, 681 with intestinal atresia, 453 with gastroschisis, 325 with exomphalos, 991 with anorectal malformation, and 517 with Hirschsprung's disease) from 264 hospitals (89 in high-income countries, 166 in middle-income countries, and nine in low-income countries) in 74 countries. Of the 3849 patients, 2231 (58·0%) were male. Median gestational age at birth was 38 weeks (IQR 36-39) and median bodyweight at presentation was 2·8 kg (2·3-3·3). Mortality among all patients was 37 (39·8%) of 93 in low-income countries, 583 (20·4%) of 2860 in middle-income countries, and 50 (5·6%) of 896 in high-income countries (p<0·0001 between all country income groups). Gastroschisis had the greatest difference in mortality between country income strata (nine [90·0%] of ten in low-income countries, 97 [31·9%] of 304 in middle-income countries, and two [1·4%] of 139 in high-income countries; p≤0·0001 between all country income groups). Factors significantly associated with higher mortality for all patients combined included country income status (low-income vs high-income countries, risk ratio 2·78 [95% CI 1·88-4·11], p<0·0001; middle-income vs high-income countries, 2·11 [1·59-2·79], p<0·0001), sepsis at presentation (1·20 [1·04-1·40], p=0·016), higher American Society of Anesthesiologists (ASA) score at primary intervention (ASA 4-5 vs ASA 1-2, 1·82 [1·40-2·35], p<0·0001; ASA 3 vs ASA 1-2, 1·58, [1·30-1·92], p<0·0001]), surgical safety checklist not used (1·39 [1·02-1·90], p=0·035), and ventilation or parenteral nutrition unavailable when needed (ventilation 1·96, [1·41-2·71], p=0·0001; parenteral nutrition 1·35, [1·05-1·74], p=0·018). Administration of parenteral nutrition (0·61, [0·47-0·79], p=0·0002) and use of a peripherally inserted central catheter (0·65 [0·50-0·86], p=0·0024) or percutaneous central line (0·69 [0·48-1·00], p=0·049) were associated with lower mortality.
Unacceptable differences in mortality exist for gastrointestinal congenital anomalies between low-income, middle-income, and high-income countries. Improving access to quality neonatal surgical care in LMICs will be vital to achieve Sustainable Development Goal 3.2 of ending preventable deaths in neonates and children younger than 5 years by 2030.
Wellcome Trust.
先天性异常是全球 5 岁以下儿童死亡的第五大主要原因。如果无法及时获得新生儿外科护理,许多胃肠道先天性异常是致命的,但很少有研究关注中低收入国家(LMICs)的这些疾病。我们比较了全球低收入、中等收入和高收入国家七种最常见的胃肠道先天性异常的结局,并确定了与死亡率相关的因素。
我们进行了一项多中心、国际前瞻性队列研究,纳入了首次因食管闭锁、先天性膈疝、肠闭锁、腹裂、脐膨出、肛门直肠畸形和先天性巨结肠就诊的年龄小于 16 岁的患者。招募时间为 2018 年 10 月至 2019 年 4 月期间至少 1 个月。我们使用 REDCap 平台收集了患者的人口统计学数据、临床状况、干预措施和结局。患者接受了原发性干预后 30 天或未接受干预后 30 天进行随访。主要结局是所有病因的住院死亡率,包括所有疾病和每种疾病的死亡率,按国家收入状况分层。我们进行了完全案例分析。
我们纳入了来自 74 个国家 264 家医院(89 家在高收入国家,166 家在中等收入国家,9 家在低收入国家)的 3849 名患者,这些患者患有 3975 种研究疾病(560 例食管闭锁,448 例先天性膈疝,681 例肠闭锁,453 例腹裂,325 例脐膨出,991 例肛门直肠畸形,517 例先天性巨结肠)。3849 名患者中,2231 名(58.0%)为男性。中位胎龄为 38 周(IQR 36-39),中位出生体重为 2.8 千克(2.3-3.3)。所有患者的死亡率为 93 例中的 37 例(39.8%),2860 例中的 583 例(20.4%),896 例中的 50 例(5.6%)(所有国家收入组之间差异有统计学意义,p<0.0001)。腹裂的死亡率在国家收入分层中差异最大(10 例中的 9 例[90.0%],304 例中的 97 例[31.9%],139 例中的 2 例[1.4%];所有国家收入组之间差异有统计学意义,p≤0.0001)。所有患者的死亡率显著相关的因素包括国家收入状况(低收入与高收入国家,风险比 2.78 [95%CI 1.88-4.11],p<0.0001;中收入与高收入国家,2.11 [1.59-2.79],p<0.0001),入院时脓毒症(1.20 [1.04-1.40],p=0.016),原发性干预时美国麻醉医师协会(ASA)评分较高(ASA 4-5 与 ASA 1-2,1.82 [1.40-2.35],p<0.0001;ASA 3 与 ASA 1-2,1.58 [1.30-1.92],p<0.0001),未使用手术安全检查表(1.39 [1.02-1.90],p=0.035),需要时无法进行通气或肠外营养(通气 1.96 [1.41-2.71],p=0.0001;肠外营养 1.35 [1.05-1.74],p=0.018)。接受肠外营养(0.61 [0.47-0.79],p=0.0002)和使用外周静脉置管(0.65 [0.50-0.86],p=0.0024)或经皮中心静脉置管(0.69 [0.48-1.00],p=0.049)与死亡率降低相关。
胃肠道先天性异常在低收入、中等收入和高收入国家之间存在不可接受的死亡率差异。改善中低收入国家获得高质量新生儿外科护理的机会对于实现可持续发展目标 3.2 至关重要,该目标是到 2030 年结束 5 岁以下儿童和新生儿可预防的死亡。
惠康信托基金会。