Department of Radiation Oncology, University of California Los Angeles, Los Angeles, CA, USA.
University of California San Diego School of Medicine, San Diego, CA, USA.
Cancer Med. 2021 Sep;10(17):5897-5906. doi: 10.1002/cam4.4139. Epub 2021 Jul 20.
Stereotactic body radiotherapy (SBRT) delivers ablative doses with excellent local control. However, implementing SBRT for abdominal and pelvic tumors has been limited by the risk for treatment-related gastrointestinal toxicity. MRI-guided radiotherapy may ameliorate these risks and increase the therapeutic ratio. We report the clinical outcomes of stereotactic MRI-guided adaptive radiotherapy (SMART) for primary and metastatic tumors in the abdomen and pelvis.
From November 2014 to August 2017, the first 106 consecutive patients with 121 tumors in the abdomen and pelvis were treated with SMART at a single institution. Of the cohort, 41.5%, 15.1%, and 43.4% had primary, locally recurrent, and oligometastatic tumors, respectively. SMART was delivered using a tri-cobalt-60 gantry with on-board 0.35 Tesla MRI with respiratory breath-hold and daily adaptive re-planning when anatomically necessary. A median of 40Gy in five fractions was prescribed. The Common Terminology Criteria for Adverse Events v.4.03 was used to score treatment-related toxicities. Local control (LC), progression-free survival (PFS), and overall survival (OS) were estimated using Kaplan-Meier method.
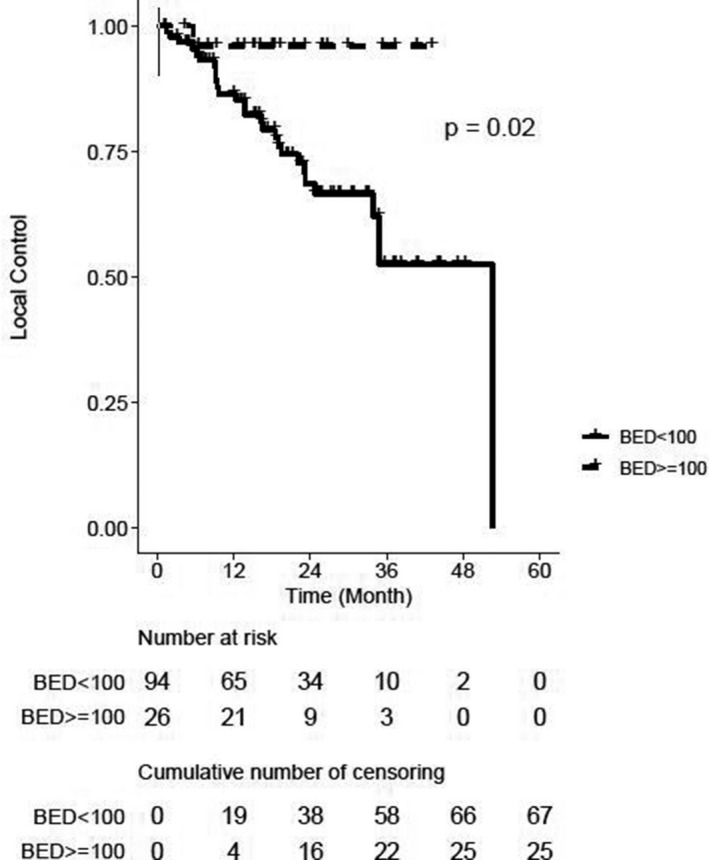
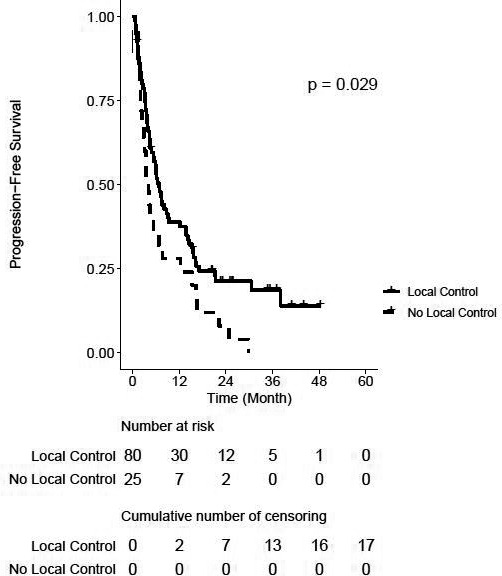
Of the 510 treatments, seventy-one (13.9%) were adapted. Fatigue, nausea, and pain were the most common acute toxicities. 0.9 and 0% of patients experienced acute grade three and four toxicities, respectively. 5.2 and 2.1% of patients experienced late grade three and four toxicities, respectively. After a median follow-up of 20.4 months, the 2-year LC rate was 74% on a per-lesion basis. Two-year LC was 96% for lesions that were treated with BED ≥100 versus 69% for BED <100 (p = 0.02). PFS was significantly different between patients with and without locally controlled tumors (2-year PFS 21 vs. 8%, p = 0.03). Two-year OS was 57% for the entire cohort.
Favorable LC and PFS outcomes were observed with minimal morbidity for tumors in the abdomen and pelvis treated with SMART. Future prospective clinical trials to validate these findings are warranted.
立体定向体部放疗(SBRT)可提供根治性剂量,局部控制效果良好。然而,由于治疗相关的胃肠道毒性风险,腹部和盆腔肿瘤的 SBRT 应用受到限制。磁共振引导放疗(MRI 引导放疗)可能改善这些风险,并提高治疗效果。我们报告了在腹部和盆腔原发和转移性肿瘤中应用立体定向 MRI 引导自适应放疗(SMART)的临床结果。
自 2014 年 11 月至 2017 年 8 月,在一家机构中,对 106 例连续 121 例腹部和盆腔肿瘤患者进行了 SMART 治疗。队列中,41.5%、15.1%和 43.4%的患者分别患有原发性、局部复发性和寡转移性肿瘤。SMART 使用三钴-60 伽玛刀和内置 0.35 特斯拉 MRI 进行治疗,采用呼吸门控和每日自适应重计划,当解剖结构有必要时进行。处方中位数为 40Gy,分 5 次。采用不良事件通用术语标准 v.4.03 对治疗相关毒性进行评分。采用 Kaplan-Meier 法估计局部控制(LC)、无进展生存期(PFS)和总生存期(OS)。
510 次治疗中有 71 次(13.9%)进行了调整。疲劳、恶心和疼痛是最常见的急性毒性。分别有 0.9%和 0%的患者出现急性 3 级和 4 级毒性。分别有 5.2%和 2.1%的患者出现迟发性 3 级和 4 级毒性。中位随访 20.4 个月后,按病变计算,2 年 LC 率为 74%。BED≥100 的病变 2 年 LC 率为 96%,BED<100 的病变为 69%(p=0.02)。LC 的患者和未 LC 的患者之间 PFS 差异有统计学意义(2 年 PFS 分别为 21%和 8%,p=0.03)。全队列的 2 年 OS 为 57%。
对于腹部和盆腔肿瘤,应用 SMART 治疗后,肿瘤局部控制率高,患者发病率低。有必要进行前瞻性临床试验来验证这些发现。