Grimbergen Guus, Eijkelenkamp Hidde, Snoeren Louk M W, Bahij Rana, Bernchou Uffe, van der Bijl Erik, Heerkens Hanne D, Binda Shawn, Ng Sylvia S W, Bouchart Christelle, Paquier Zelda, Brown Kerryn, Khor Richard, Chuter Robert, Freear Linnéa, Dunlop Alex, Mitchell Robert Adam, Erickson Beth A, Hall William A, Godoy Scripes Paola, Tyagi Neelam, de Leon Jeremiah, Tran Charles, Oh Seungjong, Renz Paul, Shessel Andrea, Taylor Edward, Intven Martijn P W, Meijer Gert J
Department of Radiation Oncology, University Medical Center Utrecht, The Netherlands.
Department of Oncology, Odense University Hospital, Denmark.
Clin Transl Radiat Oncol. 2024 May 18;47:100797. doi: 10.1016/j.ctro.2024.100797. eCollection 2024 Jul.
Treatment planning for MR-guided stereotactic body radiotherapy (SBRT) for pancreatic tumors can be challenging, leading to a wide variation of protocols and practices. This study aimed to harmonize treatment planning by developing a consensus planning protocol for MR-guided pancreas SBRT on a 1.5 T MR-Linac.
A consortium was founded of thirteen centers that treat pancreatic tumors on a 1.5 T MR-Linac. A phased planning exercise was conducted in which centers iteratively created treatment plans for two cases of pancreatic cancer. Each phase was followed by a meeting where the instructions for the next phase were determined. After three phases, a consensus protocol was reached.
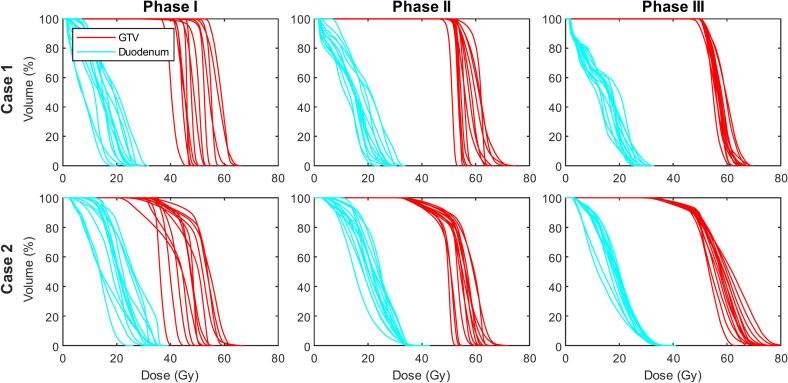
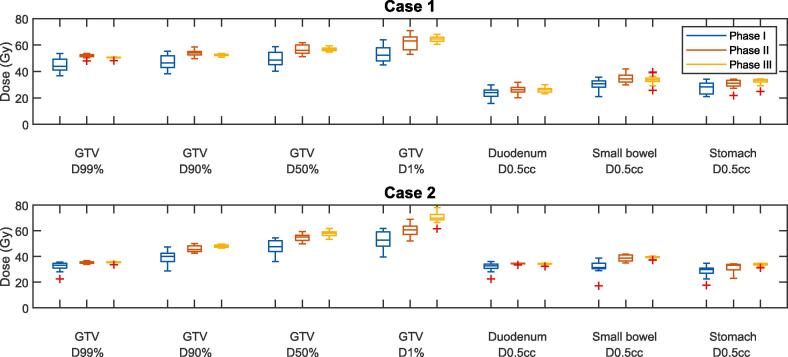
In the benchmarking phase (phase I), substantial variation between the SBRT protocols became apparent (for example, the gross tumor volume (GTV) ranged between 36.8 - 53.7 Gy for case 1, 22.6 - 35.5 Gy for case 2). The next phase involved planning according to the same basic dosimetric objectives, constraints, and planning margins (phase II), which led to a large degree of harmonization (GTV range: 47.9-53.6 Gy for case 1, 33.9-36.6 Gy for case 2). In phase III, the final consensus protocol was formulated in a treatment planning system template and again used for treatment planning. This not only resulted in further dosimetric harmonization (GTV range: 48.2-50.9 Gy for case 1, 33.5-36.0 Gy for case 2) but also in less variation of estimated treatment delivery times.
A global consensus protocol has been developed for treatment planning for MR-guided pancreatic SBRT on a 1.5 T MR-Linac. Aside from harmonizing the large variation in the current clinical practice, this protocol can provide a starting point for centers that are planning to treat pancreatic tumors on MR-Linac systems.
磁共振引导下的立体定向体部放射治疗(SBRT)用于胰腺肿瘤的治疗计划制定可能具有挑战性,导致方案和实践存在很大差异。本研究旨在通过制定1.5T MR直线加速器引导下的磁共振引导胰腺SBRT的共识计划方案,使治疗计划趋于一致。
成立了一个由13个在1.5T MR直线加速器上治疗胰腺肿瘤的中心组成的联盟。进行了一个分阶段的计划制定过程,各中心为两例胰腺癌病例反复制定治疗计划。每个阶段之后都会召开一次会议,确定下一阶段的指导方针。经过三个阶段,达成了一个共识方案。
在基准测试阶段(第一阶段),SBRT方案之间的显著差异变得明显(例如,病例1的大体肿瘤体积(GTV)范围在36.8 - 53.7Gy之间,病例2在22.6 - 35.5Gy之间)。下一阶段根据相同的基本剂量学目标、限制条件和计划边界进行计划制定(第二阶段),这导致了很大程度的一致性(病例1的GTV范围:47.9 - 53.6Gy,病例2为33.9 - 36.6Gy)。在第三阶段,在治疗计划系统模板中制定了最终的共识方案,并再次用于治疗计划制定。这不仅进一步实现了剂量学上的一致性(病例1的GTV范围:48.2 - 50.9Gy,病例2为33.5 - 36.0Gy),而且估计的治疗实施时间的差异也更小。
已制定了一项关于1.5T MR直线加速器引导下的磁共振引导胰腺SBRT治疗计划的全球共识方案。除了使当前临床实践中的巨大差异趋于一致外,该方案还可为计划在MR直线加速器系统上治疗胰腺肿瘤的中心提供一个起点。