Amundsen Erik K, Binde Christina, Christensen Erik E, Klingenberg Olav, Kvale Dag, Holten Aleksander R
Department of Medical Biochemistry, Oslo University Hospital, Oslo, Norway.
Department of Life Sciences and Health, Oslo Metropolitan University, Oslo, Norway.
Crit Care Explor. 2021 Jul 16;3(7):e0490. doi: 10.1097/CCE.0000000000000490. eCollection 2021 Jul.
Increase of nucleated RBCs in peripheral blood has been shown to be predictive of mortality in ICU patients. The aim of this study was to explore the prognostic value of nucleated RBCs in the first blood sample taken at admission to the emergency department from patients with suspected sepsis.
Single-center prospective cohort study.
Emergency department.
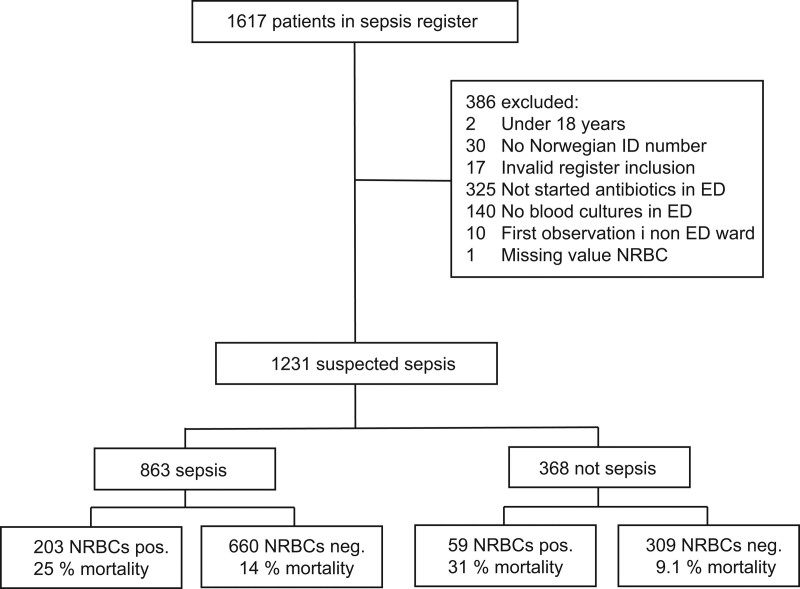
One-thousand two-hundred thirty-one consecutive adult patients with suspected sepsis were included in a prospective quality register-based cohort study. Inclusion criteria were as follows: patients received in rapid response team with blood cultures taken and immediate antibiotics given in the emergency department.
Not applicable.
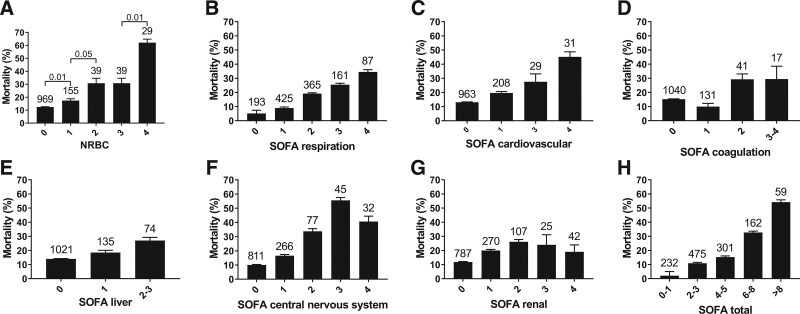
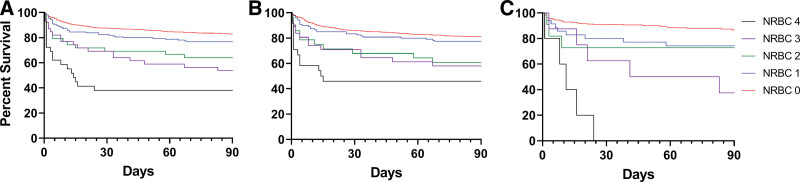
Nucleated RBCs, Sequential Organ Failure Assessment score, Quick Sequential Organ Failure Assessment, Charlson Comorbidity Index, and commonly used laboratory tests measured in the emergency department were compared with 30-day mortality. Nvaucleated RBC counts were divided into five groups, called "Nucleated RBC score," according to nucleated RBC count levels and analyzed with logistic regression together with the Sequential Organ Failure Assessment score and Charlson Comorbidity Index. Of the 262 patients with nucleated RBCs equal to or higher than the detection limit (0.01 × 10/L), 26% died within 30 days, compared with 12% of the 969 patients with nucleated RBCs below the detection limit ( < 0.0001). Mortality was significantly higher for each increase in Nucleated RBC score, except from score 2 to 3, and was 62% in the highest group. In multivariate logistic regression, odds ratios for 30-day mortality were as follows: Nucleated RBC score: 1.33 (95% CI, 1.13-1.56), Sequential Organ Failure Assessment score: 1.32 (1.29-1.56), and Charlson Comorbidity Index: 1.17 (1.09-1.25).
Most patients with suspected sepsis in emergency department had undetectable nucleated RBCs at admission to the emergency department. However, increased nucleated RBCs significantly predicted 30-day mortality. Nucleated RBCs may provide additional prognostic information to Sequential Organ Failure Assessment score and other laboratory tests.
外周血中有核红细胞增多已被证明可预测重症监护病房患者的死亡率。本研究的目的是探讨在急诊科对疑似脓毒症患者入院时采集的第一份血样中有核红细胞的预后价值。
单中心前瞻性队列研究。
急诊科。
1231例连续的疑似脓毒症成年患者被纳入一项基于前瞻性质量登记的队列研究。纳入标准如下:患者由快速反应团队接诊,在急诊科采集血培养并立即给予抗生素治疗。
不适用。
将急诊科测量的有核红细胞、序贯器官衰竭评估评分、快速序贯器官衰竭评估、查尔森合并症指数及常用实验室检查结果与30天死亡率进行比较。根据有核红细胞计数水平将有核红细胞计数分为五组,称为“有核红细胞评分”,并与序贯器官衰竭评估评分和查尔森合并症指数一起进行逻辑回归分析。在262例有核红细胞等于或高于检测限(0.01×10/L)的患者中,26%在30天内死亡,而在969例有核红细胞低于检测限(<0.0001)的患者中,这一比例为12%。除了从评分2到评分3外,有核红细胞评分每增加一级,死亡率均显著升高,最高组的死亡率为62%。在多因素逻辑回归分析中,30天死亡率的比值比分别为:有核红细胞评分:1.33(95%CI,1.13 - 1.56),序贯器官衰竭评估评分:1.32(1.29 - 1.56),查尔森合并症指数:1.17(1.