Vekaria Bindu, Overton Christopher, Wiśniowski Arkadiusz, Ahmad Shazaad, Aparicio-Castro Andrea, Curran-Sebastian Jacob, Eddleston Jane, Hanley Neil A, House Thomas, Kim Jihye, Olsen Wendy, Pampaka Maria, Pellis Lorenzo, Ruiz Diego Perez, Schofield John, Shryane Nick, Elliot Mark J
Department of Mathematics, University of Manchester, Oxford Road, Manchester, M13 9PL, UK.
Division of Informatics, Imaging and Data Science, Faculty of Biology, Medicine and Health, University of Manchester, Manchester Academic Health Science Centre, Oxford Road, Manchester, M13 9PL, UK.
BMC Infect Dis. 2021 Jul 22;21(1):700. doi: 10.1186/s12879-021-06371-6.
Predicting hospital length of stay (LoS) for patients with COVID-19 infection is essential to ensure that adequate bed capacity can be provided without unnecessarily restricting care for patients with other conditions. Here, we demonstrate the utility of three complementary methods for predicting LoS using UK national- and hospital-level data.
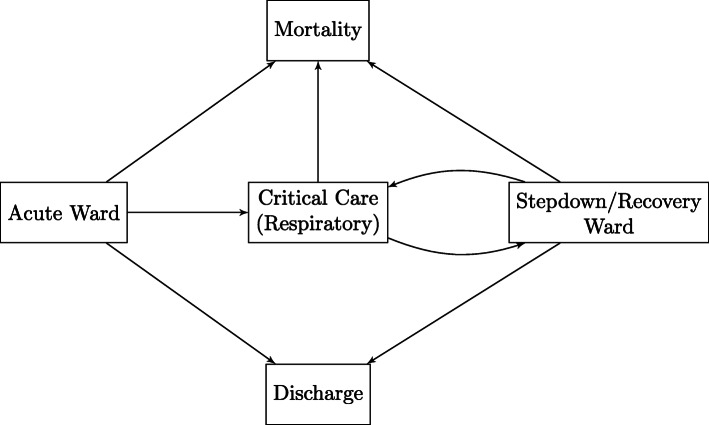
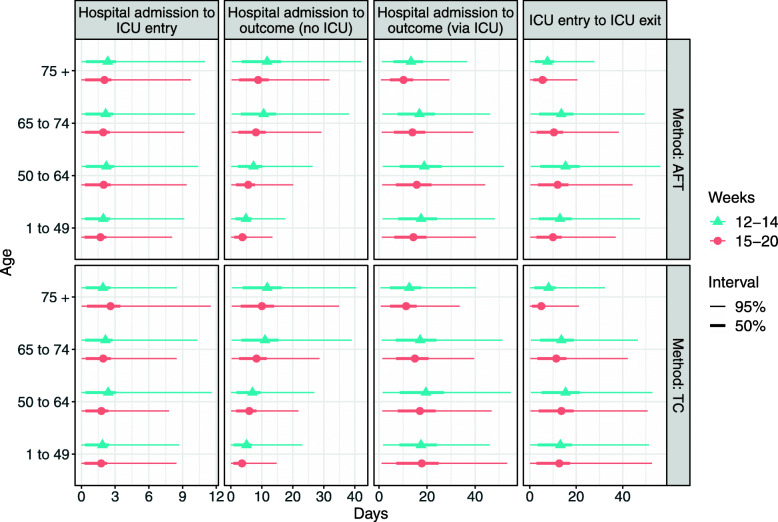
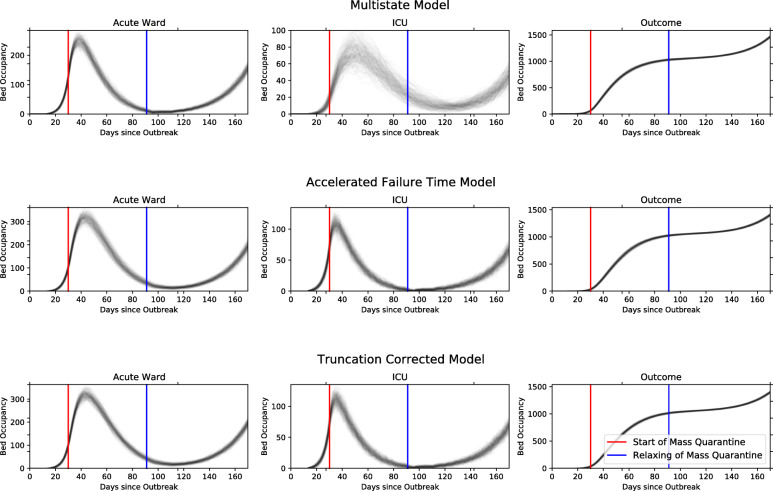
On a national scale, relevant patients were identified from the COVID-19 Hospitalisation in England Surveillance System (CHESS) reports. An Accelerated Failure Time (AFT) survival model and a truncation corrected method (TC), both with underlying Weibull distributions, were fitted to the data to estimate LoS from hospital admission date to an outcome (death or discharge) and from hospital admission date to Intensive Care Unit (ICU) admission date. In a second approach we fit a multi-state (MS) survival model to data directly from the Manchester University NHS Foundation Trust (MFT). We develop a planning tool that uses LoS estimates from these models to predict bed occupancy.
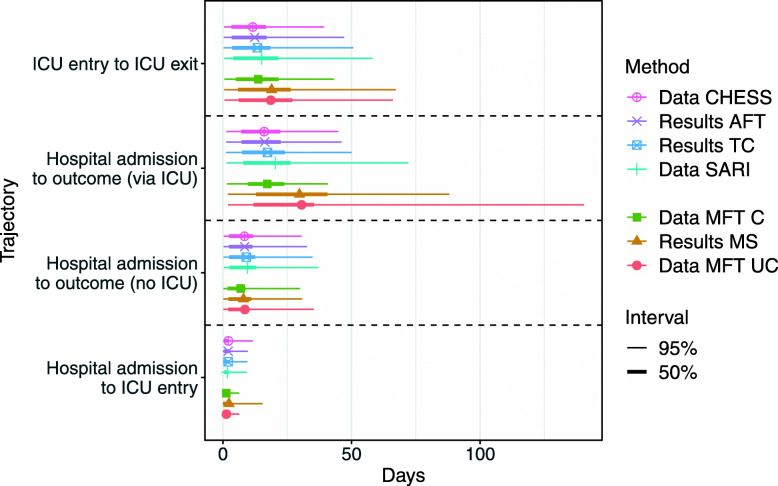
All methods produced similar overall estimates of LoS for overall hospital stay, given a patient is not admitted to ICU (8.4, 9.1 and 8.0 days for AFT, TC and MS, respectively). Estimates differ more significantly between the local and national level when considering ICU. National estimates for ICU LoS from AFT and TC were 12.4 and 13.4 days, whereas in local data the MS method produced estimates of 18.9 days.
Given the complexity and partiality of different data sources and the rapidly evolving nature of the COVID-19 pandemic, it is most appropriate to use multiple analysis methods on multiple datasets. The AFT method accounts for censored cases, but does not allow for simultaneous consideration of different outcomes. The TC method does not include censored cases, instead correcting for truncation in the data, but does consider these different outcomes. The MS method can model complex pathways to different outcomes whilst accounting for censoring, but cannot handle non-random case missingness. Overall, we conclude that data-driven modelling approaches of LoS using these methods is useful in epidemic planning and management, and should be considered for widespread adoption throughout healthcare systems internationally where similar data resources exist.
预测新型冠状病毒肺炎(COVID-19)感染患者的住院时长对于确保能够提供足够的床位,同时又不会不必要地限制对患有其他疾病患者的治疗至关重要。在此,我们展示了三种使用英国国家和医院层面数据预测住院时长的互补方法的效用。
在全国范围内,从英格兰COVID-19住院监测系统(CHESS)报告中识别相关患者。将具有潜在威布尔分布的加速失效时间(AFT)生存模型和截断校正方法(TC)应用于数据,以估计从入院日期到结局(死亡或出院)以及从入院日期到重症监护病房(ICU)入院日期的住院时长。在第二种方法中,我们将多状态(MS)生存模型应用于直接来自曼彻斯特大学国民保健服务基金会信托基金(MFT)的数据。我们开发了一种规划工具,该工具使用这些模型的住院时长估计值来预测床位占用情况。
对于未入住ICU的患者,所有方法对总体住院时长的总体估计相似(AFT、TC和MS方法分别为8.4天、9.1天和8.0天)。考虑ICU时,地方和国家层面的估计差异更为显著。AFT和TC方法对ICU住院时长的国家层面估计分别为12.4天和13.4天,而在地方数据中,MS方法得出的估计值为18.9天。
鉴于不同数据源的复杂性和局限性以及COVID-19大流行的快速演变性质,对多个数据集使用多种分析方法最为合适。AFT方法考虑了删失病例,但不允许同时考虑不同结局。TC方法不包括删失病例,而是对数据中的截断进行校正,但确实考虑了这些不同结局。MS方法可以对通往不同结局的复杂路径进行建模,同时考虑删失情况,但无法处理非随机的病例缺失。总体而言,我们得出结论,使用这些方法对住院时长进行数据驱动的建模方法在疫情规划和管理中很有用,并且在国际上存在类似数据资源的整个医疗系统中应考虑广泛采用。