Stanski Natalja L, Wong Hector R, Basu Rajit K, Cvijanovich Natalie Z, Fitzgerald Julie C, Weiss Scott L, Bigham Michael T, Jain Parag N, Schwarz Adam, Lutfi Riad, Nowak Jeffrey, Allen Geoffrey L, Thomas Neal J, Grunwell Jocelyn R, Quasney Michael, Haileselassie Bereketeab, Chawla Lakhmir S, Goldstein Stuart L
Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio, USA.
Department of Pediatrics, University of Cincinnati College of Medicine, Cincinnati, Ohio, USA.
Kidney Int Rep. 2021 May 1;6(7):1858-1867. doi: 10.1016/j.ekir.2021.04.022. eCollection 2021 Jul.
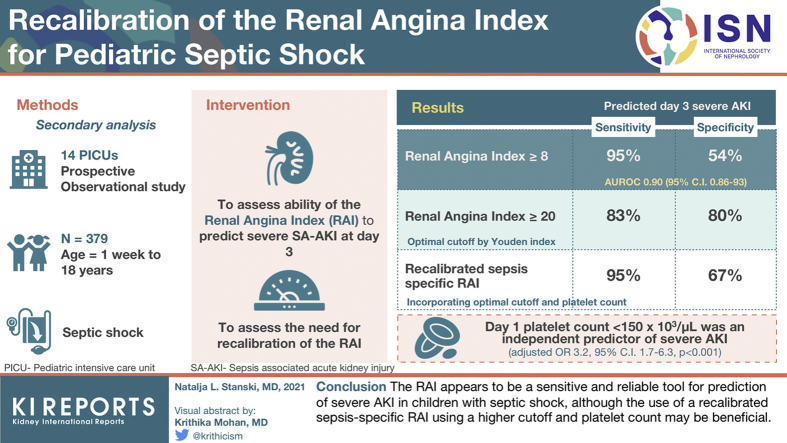
Sepsis-associated acute kidney injury (AKI) is a common diagnosis in children that is associated with poor outcomes. The lack of therapeutic options once present makes early identification of at-risk patients essential. The renal angina index (RAI) has been previously validated to predict severe AKI in heterogeneous populations of critically ill children. The performance of this score specifically in children with septic shock is unknown.
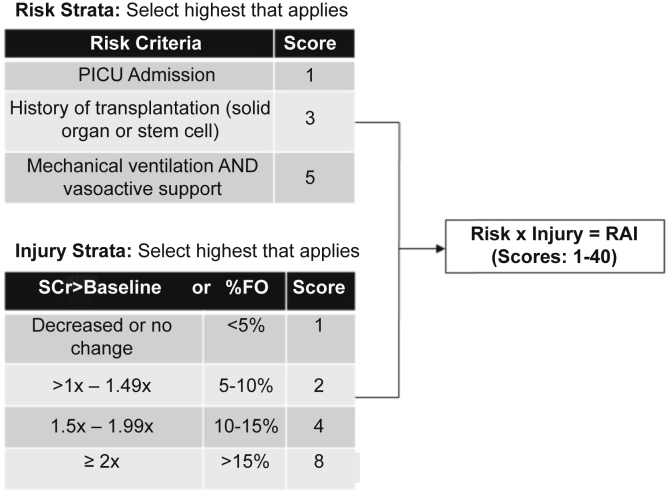
A secondary analysis of a multicenter, prospective, observational study of 379 children with septic shock to determine the ability of the RAI to predict severe AKI at day 3, and to assess for the potential need for recalibration of the RAI in this unique subset of patients.
At the original cutoff of ≥8, the RAI predicted day 3 severe AKI with an area under the receiving operating characteristic (AUROC) curve 0.90 (95% confidence interval [CI]: 0.86 to 93), 95% sensitivity, and 54% specificity. A Youden's index identified a higher optimal cutoff of ≥20 (sensitivity 83%, specificity 80%), and day 1 platelet count <150 × 10/μl was an independent predictor of severe AKI (adjusted odds ratio: 3.2; 95% CI: 1.7 to 6.3; < 0.001). Recalibration of the RAI to include platelet count and this new threshold restored the sensitivity of the original ≥8 threshold (95%), while improving its specificity (69%).
The RAI appears to be a sensitive and reliable tool for prediction of severe AKI in children with septic shock, although the use of a recalibrated sepsis-specific RAI using a higher cutoff and platelet count may be beneficial.
脓毒症相关急性肾损伤(AKI)是儿童常见的诊断,与不良预后相关。一旦出现则缺乏治疗选择,因此早期识别高危患者至关重要。肾绞痛指数(RAI)先前已被验证可预测危重症儿童异质性群体中的严重AKI。该评分在感染性休克儿童中的具体表现尚不清楚。
对一项多中心、前瞻性、观察性研究进行二次分析,该研究纳入了379例感染性休克儿童,以确定RAI预测第3天严重AKI的能力,并评估在这一独特患者亚组中重新校准RAI的潜在必要性。
在最初的截断值≥8时,RAI预测第3天严重AKI的受试者工作特征曲线(AUROC)下面积为0.90(95%置信区间[CI]:0.86至0.93),敏感性为95%,特异性为54%。约登指数确定了更高的最佳截断值≥20(敏感性83%,特异性80%),且第1天血小板计数<150×10⁹/μl是严重AKI的独立预测因素(调整优势比:3.2;95%CI:1.7至6.3;P<0.001)。将血小板计数和这一新阈值纳入重新校准RAI,恢复了原始≥8阈值的敏感性(95%),同时提高了其特异性(69%)。
RAI似乎是预测感染性休克儿童严重AKI的敏感且可靠的工具,尽管使用更高截断值和血小板计数重新校准的脓毒症特异性RAI可能有益。