Goldstein Stuart L, Krallman Kelli A, Roy Jean-Philippe, Collins Michaela, Chima Ranjit S, Basu Rajit K, Chawla Lakhmir, Fei Lin
Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio, USA.
Lurie Children's Hospital, Chicago Illinois, USA.
Kidney Int Rep. 2023 Sep 22;8(12):2690-2700. doi: 10.1016/j.ekir.2023.09.019. eCollection 2023 Dec.
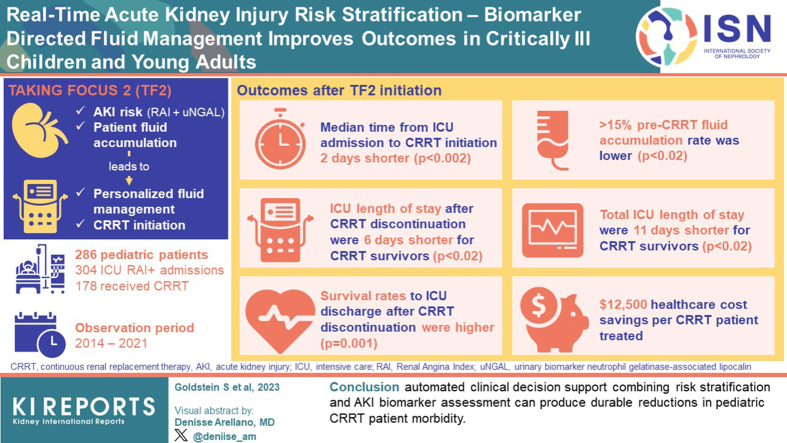
Critically ill admitted patients are at high risk of acute kidney injury (AKI). The renal angina index (RAI) and urinary biomarker neutrophil gelatinase-associated lipocalin (uNGAL) can aid in AKI risk assessment. We implemented the Trial in AKI using NGAL and Fluid Overload to optimize CRRT Use (TAKING FOCUS 2; TF2) to personalize fluid management and continuous renal replacement therapy (CRRT) initiation based on AKI risk and patient fluid accumulation. We compared outcomes pre-TF2 and post-TF2 initiation.
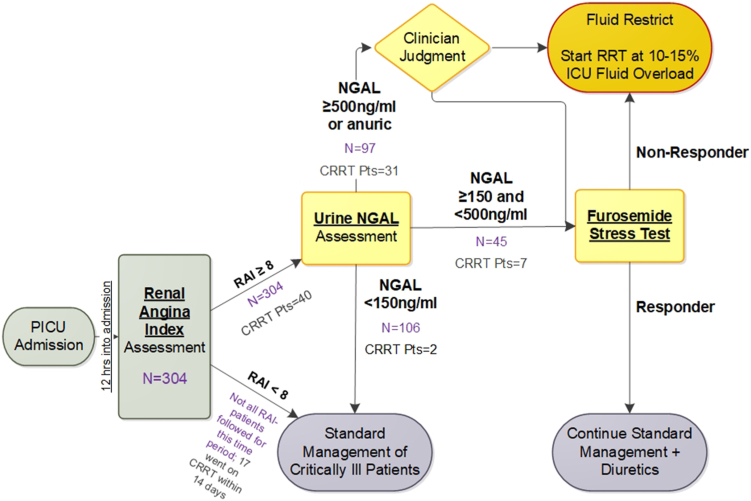
Patients admitted from July 2017 were followed-up prospectively with the following: (i) an automated RAI result at 12 hours of admission, (ii) a conditional uNGAL order for RAI ≥8, and (iii) a CRRT initiation goal at 10% to 15% weight-based fluid accumulation.
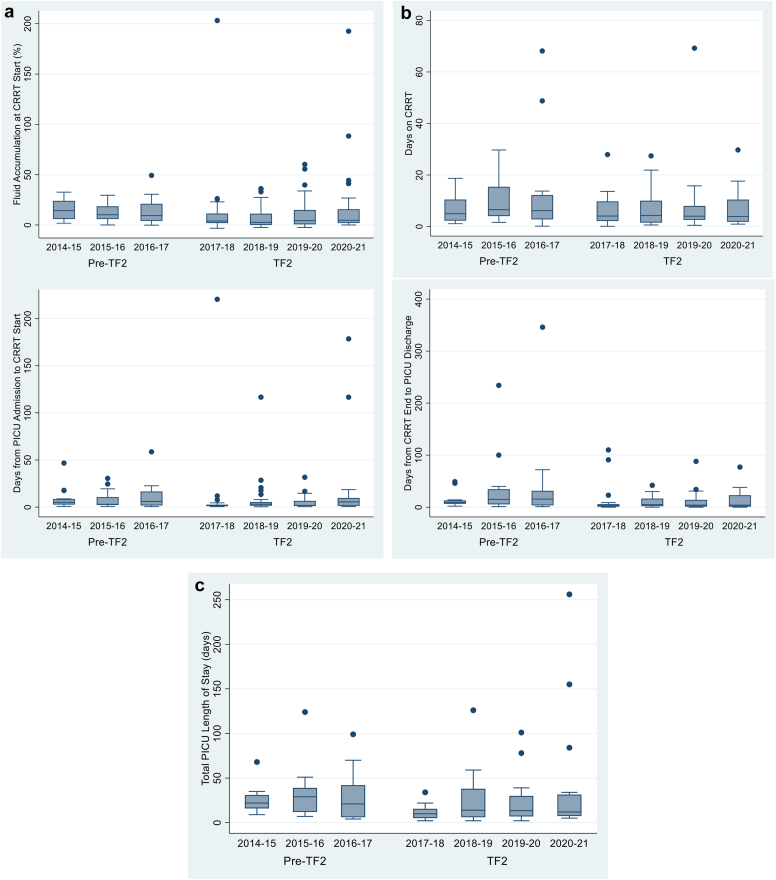
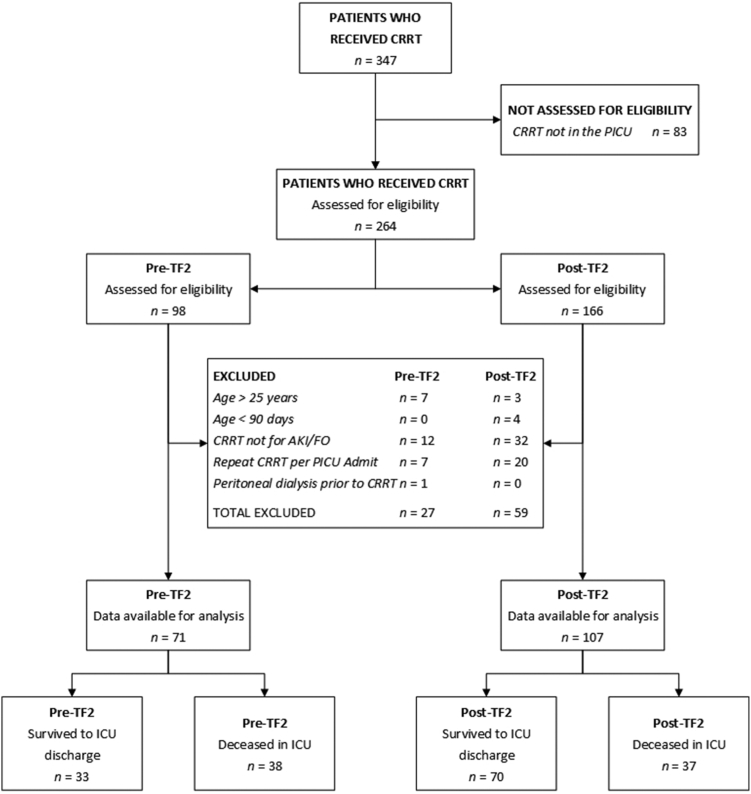
A total of 286 patients comprised 304 intensive care unit (ICU) RAI+ admissions; 178 patients received CRRT over the observation period (2014-2021). Median time from ICU admission to CRRT initiation was 2 days shorter ( < 0.002), and ≥15% pre-CRRT fluid accumulation rate was lower in the TF2 era ( < 0.02). TF2 ICU length of stay (LOS) after CRRT discontinuation and total ICU LOS were 6 and 11 days shorter for CRRT survivors (both < 0.02). Survival rates to ICU discharge after CRRT discontinuation were higher in the TF2 era ( = 0.001). These associations persisted in each TF2 year; we estimate a conservative $12,500 health care cost savings per CRRT patient treated after TF2 implementation.
We suggest that automated clinical decision support (CDS) combining risk stratification and AKI biomarker assessment can produce durable reductions in pediatric CRRT patient morbidity.
危重症入院患者发生急性肾损伤(AKI)的风险很高。肾绞痛指数(RAI)和尿生物标志物中性粒细胞明胶酶相关脂质运载蛋白(uNGAL)有助于评估AKI风险。我们开展了使用NGAL和液体超负荷优化CRRT使用的AKI试验(TAKING FOCUS 2;TF2),以根据AKI风险和患者液体蓄积情况实现个性化液体管理和启动连续性肾脏替代治疗(CRRT)。我们比较了TF2启动前后的结果。
对2017年7月入院的患者进行前瞻性随访,包括:(i)入院12小时时的自动RAI结果,(ii)RAI≥8时的条件性uNGAL检测医嘱,以及(iii)基于体重的液体蓄积达到10%至15%时的CRRT启动目标。
共有286例患者构成304次重症监护病房(ICU)RAI阳性入院;178例患者在观察期(2014 - 2021年)接受了CRRT治疗。从ICU入院到开始CRRT的中位时间缩短了2天(<0.002),TF2时代CRRT前≥15%的液体蓄积率更低(<0.02)。对于CRRT幸存者,CRRT停止后的TF2 ICU住院时间(LOS)和总ICU LOS分别缩短了6天和11天(均<0.02)。TF2时代CRRT停止后至ICU出院的生存率更高(=0.001)。这些关联在TF2的每一年都持续存在;我们估计,在实施TF2后,每位接受CRRT治疗的患者可节省保守估计的12,500美元医疗费用。
我们建议,结合风险分层和AKI生物标志物评估的自动化临床决策支持(CDS)可以持续降低儿科CRRT患者的发病率。