Department of Obstetrics and Gynecology, University Medical Centre Groningen, Groningen, The Netherlands.
Department of Genetics, EUROCAT Registration Northern Netherlands, University Medical Centre Groningen, Groningen, The Netherlands.
Paediatr Perinat Epidemiol. 2021 Nov;35(6):654-663. doi: 10.1111/ppe.12792. Epub 2021 Jul 30.
Perinatal mortality in foetuses/children with congenital anomalies remains high. Prenatal diagnosis, essential for risk assessment and organisation of perinatal/postnatal care, offers parents the opportunity to consider the termination of pregnancy. In times of quick changes in prenatal screening programmes, it is relevant to evaluate the effect of prenatal screening on perinatal mortality rates.
The objective of this study was to study trends in early foetal and perinatal mortality associated with congenital anomalies before/after the introduction of the Dutch prenatal screening programme.
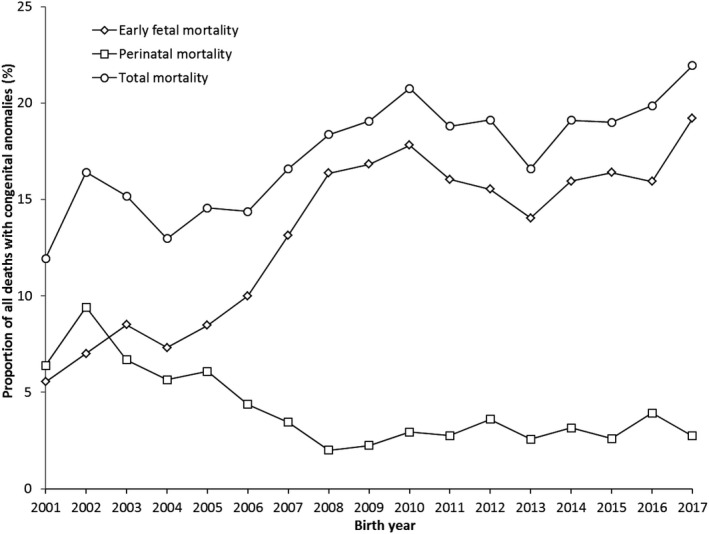
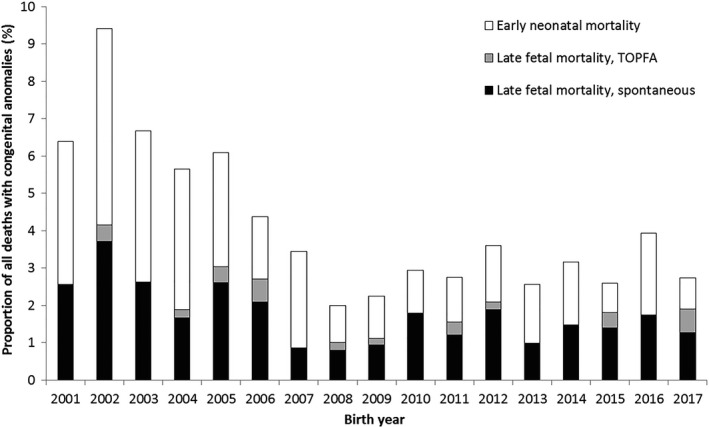
This population-based cohort study included 8535 foetuses/neonates with congenital anomalies born in the Northern Netherlands between 2001 and 2017. Total deaths were defined as sum of early foetal (before 24 weeks' gestation) and perinatal deaths (from 24 weeks' gestation till day 7 post-partum). Foetal deaths were categorised into spontaneous or elective termination of pregnancy for foetal anomalies (TOPFA). Trends in total mortality as well as early foetal and perinatal mortality were studied. Joinpoint regression was used to calculate the average annual percentage chance (AAPC) and identify linear trends in mortality within subperiods.
Total and perinatal mortality were 17% and 4%. Total mortality was higher in abnormal karyotype and central nervous system anomalies. We observed an increase in total mortality over time: 11.9% in 2001 versus 21.9% in 2017 (AAPC 2.6, 95% confidence interval [CI] 1.5, 3.7), caused by an increase in early foetal mortality from 5.5% to 19.2% (AAPC 8.7, 95% CI 4.7, 12.9) and a decrease in perinatal mortality from 6.4% to 2.7% (AAPC -5.6, 95% CI -10.0, -1.0). The increase in early foetal mortality reflects an increase in TOPFA from 3.6% to 16.9% (AAPC 8.3, 95% CI 4.2, 12.7), mostly occurring at 13-14 and 20-23 weeks' gestation.
The introduction of the prenatal screening programme led to a decrease in perinatal mortality among foetuses and neonates with congenital anomalies and a marked increase in early foetal mortality before 24 weeks' gestation due to higher rates of TOPFA.
先天性异常胎儿/儿童的围产儿死亡率仍然很高。产前诊断对于风险评估和围产期/产后护理的组织至关重要,它为父母提供了考虑终止妊娠的机会。在产前筛查计划快速变化的时代,评估产前筛查对围产儿死亡率的影响是很重要的。
本研究的目的是研究在荷兰产前筛查计划引入前后与先天性异常相关的早期胎儿和围产儿死亡率的趋势。
本研究为基于人群的队列研究,纳入了 2001 年至 2017 年期间在荷兰北部出生的 8535 例先天性异常胎儿/新生儿。总死亡定义为早期胎儿(24 周前)和围产儿(24 周至产后 7 天)死亡的总和。胎儿死亡分为自发或因胎儿异常(TOPFA)而选择性终止妊娠。研究了总死亡率以及早期胎儿和围产儿死亡率的趋势。使用 Joinpoint 回归计算死亡率在亚时段内的平均年度百分比变化(AAPC)和线性趋势。
总死亡率和围产儿死亡率分别为 17%和 4%。异常核型和中枢神经系统异常的总死亡率较高。我们观察到总死亡率随时间的增加:2001 年为 11.9%,2017 年为 21.9%(AAPC2.6,95%置信区间[CI]1.5,3.7),这是由于早期胎儿死亡率从 5.5%增加到 19.2%(AAPC8.7,95%CI4.7,12.9)和围产儿死亡率从 6.4%下降到 2.7%(AAPC-5.6,95%CI-10.0,-1.0)所致。早期胎儿死亡率的增加反映了 TOPFA 从 3.6%增加到 16.9%(AAPC8.3,95%CI4.2,12.7),主要发生在 13-14 周和 20-23 周。
产前筛查计划的引入导致先天性异常胎儿和新生儿的围产儿死亡率下降,而 24 周前的早期胎儿死亡率显著增加,这主要是由于 TOPFA 的发生率较高。