Baycrest Health Sciences Centre, Toronto, Ontario, Canada.
Department of Psychology, University of Victoria, British Columbia, Canada.
J Gerontol B Psychol Sci Soc Sci. 2022 Feb 3;77(2):341-350. doi: 10.1093/geronb/gbab097.
Our aim was to validate the online Brain Health Assessment (BHA) for detection of amnestic mild cognitive impairment (aMCI) compared to gold-standard neuropsychological assessment. We compared the diagnostic accuracy of the BHA to the Montreal Cognitive Assessment (MoCA).
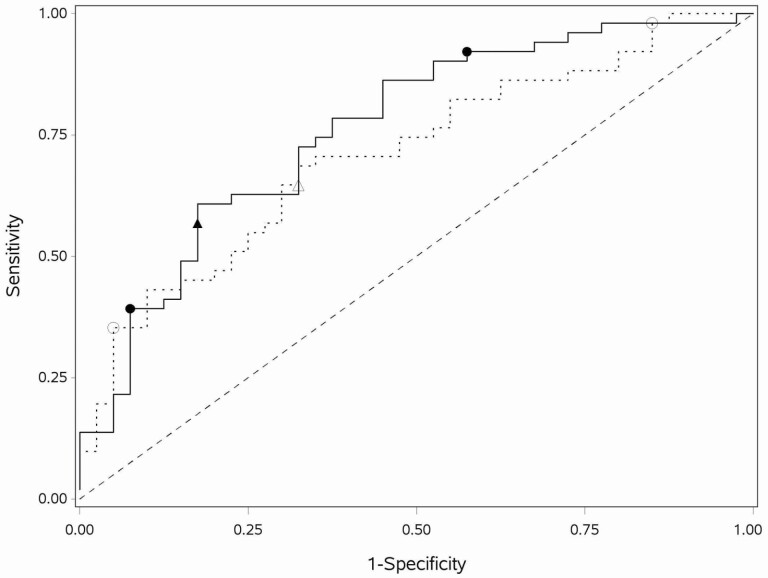
Using a cross-sectional design, community-dwelling older adults completed a neuropsychological assessment, were diagnosed as normal cognition (NC) or aMCI, and completed the BHA and MoCA. Both logistic regression (LR) and penalized logistic regression (PLR) analyses determined BHA and demographic variables predicting aMCI; MoCA variables were similarly modeled. Diagnostic accuracy was compared using area under the receiver operating characteristic curve (ROC AUC) analyses.
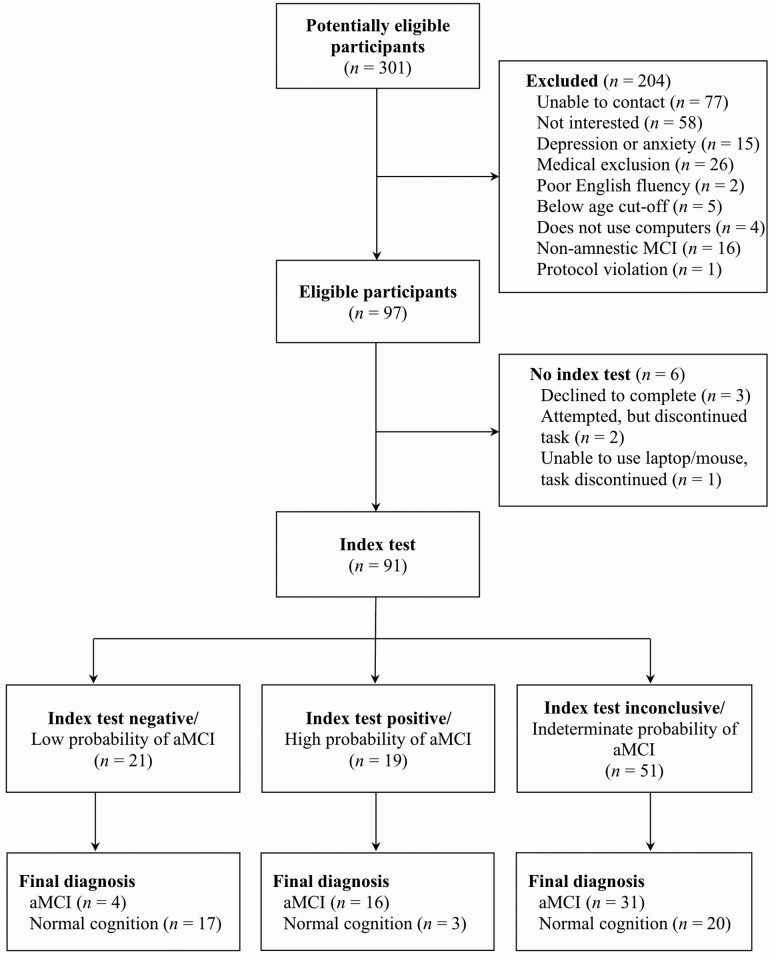
Ninety-one participants met inclusion criteria (51 aMCI, 40 NC). PLR modeling for the BHA indicated Face-Name Association, Spatial Working Memory, and age-predicted aMCI (ROC AUC = 0.76; 95% confidence interval [CI]: 0.66-0.86). Optimal cut-points resulted in 21% classified as aMCI (positive), 23% negative, and 56% inconclusive. For the MoCA, digits, abstraction, delayed recall, orientation, and age predicted aMCI (ROC AUC = 0.71; 95% CI: 0.61-0.82). Optimal cut-points resulted in 22% classified positive, 8% negative, and 70% inconclusive (LR results presented within). The BHA model classified fewer participants into the inconclusive category and more as negative for aMCI, compared to the MoCA model (Stuart-Maxwell p = .004).
The self-administered BHA provides similar detection of aMCI as a clinician-administered screener (MoCA), with fewer participants classified inconclusively. The BHA has the potential to save practitioners time and decrease unnecessary referrals for a comprehensive assessment to determine the presence of aMCI.
本研究旨在验证在线脑健康评估(BHA)在诊断遗忘型轻度认知障碍(aMCI)方面的准确性,并与金标准神经心理学评估进行比较。我们比较了 BHA 和蒙特利尔认知评估(MoCA)的诊断准确性。
采用横断面设计,社区居住的老年人完成神经心理学评估,被诊断为正常认知(NC)或 aMCI,并完成 BHA 和 MoCA。逻辑回归(LR)和惩罚逻辑回归(PLR)分析确定了预测 aMCI 的 BHA 和人口统计学变量;MoCA 变量也采用类似的模型进行分析。通过接受者操作特征曲线(ROC AUC)分析比较诊断准确性。
91 名参与者符合纳入标准(51 名 aMCI,40 名 NC)。BHA 的 PLR 模型表明,面孔-名称关联、空间工作记忆和年龄预测 aMCI(ROC AUC = 0.76;95%置信区间 [CI]:0.66-0.86)。最佳截断点导致 21%的患者被归类为 aMCI(阳性),23%为阴性,56%为不确定。对于 MoCA,数字、抽象、延迟回忆、定向和年龄预测 aMCI(ROC AUC = 0.71;95% CI:0.61-0.82)。最佳截断点导致 22%的患者被归类为阳性,8%为阴性,70%为不确定(LR 结果在文中呈现)。与 MoCA 模型相比,BHA 模型将更少的参与者归类为不确定类别,更多的患者归类为 aMCI 阴性(Stuart-Maxwell p =.004)。
自我管理的 BHA 与临床医生管理的筛查工具(MoCA)在检测 aMCI 方面具有相似的效果,但将更少的参与者归类为不确定。BHA 有可能为从业者节省时间,并减少不必要的转介,以进行全面评估以确定是否存在 aMCI。