Leon H. Charney Division of Cardiology, Department of Medicine, Soter Center for Women's Cardiovascular Research, New York University School of Medicine, New York, NY, United States of America.
Duke Clinical Research Institute, Durham, NC, United States of America.
PLoS One. 2021 Aug 2;16(8):e0255462. doi: 10.1371/journal.pone.0255462. eCollection 2021.
Optimal medical therapy after myocardial infarction with nonobstructive coronary arteries (MINOCA; <50% stenosis) is uncertain. We evaluated variability in discharge prescription of angiotensin-converting enzyme inhibitors / angiotensin receptor blockers (ACEI/ARB) and beta-blockers (BB) to MINOCA patients between hospitals to assess physician equipoise about secondary prevention.
Patients with MINOCA between 2007-2014 were identified in the NCDR Chest Pain-MI Registry. Those with prior revascularization or missing demographic, angiographic, or medication data were excluded. Analysis was limited to high-volume hospitals with ≥20 MINOCA total discharges. Discharge prescriptions for ACEI/ARB and BB after MINOCA were analyzed for each hospital. Clinical data on left ventricular ejection fraction (LVEF), glomerular filtration rate (GFR), and diabetes mellitus status were extracted to identify other indications for ACEI/ARB or BB.
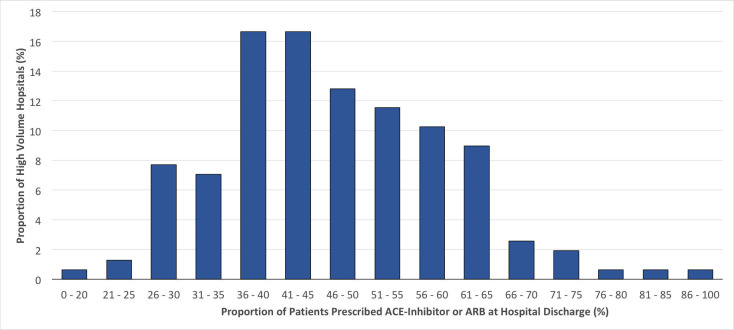
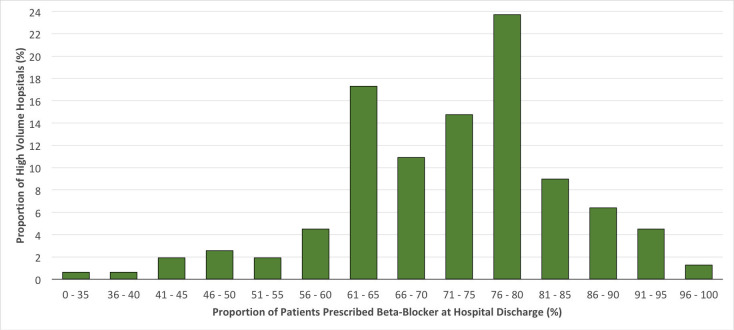
Clinical data were available for 17,849 MINOCA patients, of whom 8,752 (49%) had LVEF <40%, GFR ≤60 mL/min, and/or diabetes. 5,913 patients without one of these indications for ACEI/ARB or BB were discharged from 156 high-volume hospitals. At discharge, ACEI/ARB was prescribed to between 16.0% and 88.8% of MINOCA patients (median 45.6%, IQR 38.0%-56.5%) and BB to between 28.0% and 97.5% (median 74.1%, IQR 64.7%-80.0%).
There is marked variability between hospitals in the proportions of patients receiving ACEI/ARB and BB after hospitalization for MINOCA, suggesting clinical equipoise about the routine use of these agents. Randomized clinical trials are necessary to establish the benefit of ACEI/ARB and BB to improve outcomes after MINOCA.
心肌梗死后非阻塞性冠状动脉(MINOCA;<50%狭窄)的最佳药物治疗仍不确定。我们评估了医院间 MINOCA 患者出院时血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂(ACEI/ARB)和β受体阻滞剂(BB)处方的差异,以评估医生对二级预防的意见是否一致。
在 NCDR 胸痛-MI 登记处确定 2007-2014 年期间的 MINOCA 患者。排除有再血管化或缺少人口统计学、血管造影或药物数据的患者。分析仅限于有≥20 例 MINOCA 总出院量的高容量医院。分析每个医院 MINOCA 后的 ACEI/ARB 和 BB 出院处方。提取左心室射血分数(LVEF)、肾小球滤过率(GFR)和糖尿病状态的临床数据,以确定 ACEI/ARB 或 BB 的其他适应证。
MINOCA 患者的临床数据可用于 17849 例患者,其中 8752 例(49%)LVEF<40%、GFR≤60 mL/min 和/或糖尿病。无 ACEI/ARB 或 BB 适应证的 5913 例患者从 156 家高容量医院出院。出院时,ACEI/ARB 被处方给 MINOCA 患者的比例为 16.0%至 88.8%(中位数 45.6%,IQR 38.0%至 56.5%),BB 的比例为 28.0%至 97.5%(中位数 74.1%,IQR 64.7%至 80.0%)。
MINOCA 住院患者接受 ACEI/ARB 和 BB 的比例在医院之间存在显著差异,表明医生对这些药物的常规使用存在意见分歧。需要进行随机临床试验来确定 ACEI/ARB 和 BB 对改善 MINOCA 后结局的益处。