Department of Radiation Oncology, University Medical Centre Mannheim, University of Heidelberg, Theodor-Kutzer-Ufer 1-3, 68167, Mannheim, Germany.
Department of Radiation Oncology, University Hospital Bonn, University of Bonn, Bonn, Germany.
Radiat Oncol. 2021 Aug 4;16(1):145. doi: 10.1186/s13014-021-01872-9.
Hypofractionation is increasingly being applied in radiotherapy for prostate cancer, requiring higher accuracy of daily treatment deliveries than in conventional image-guided radiotherapy (IGRT). Different adaptive radiotherapy (ART) strategies were evaluated with regard to dosimetric benefits.
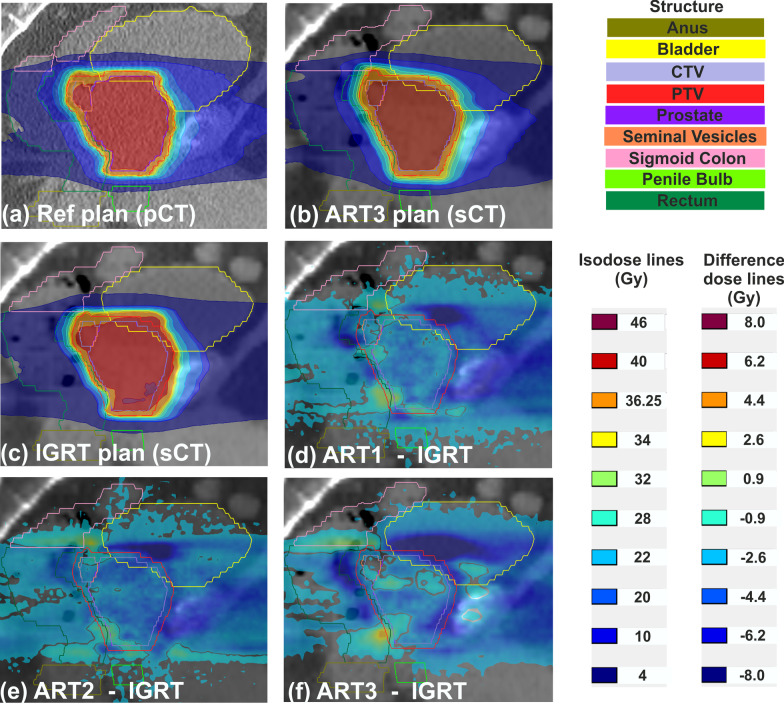
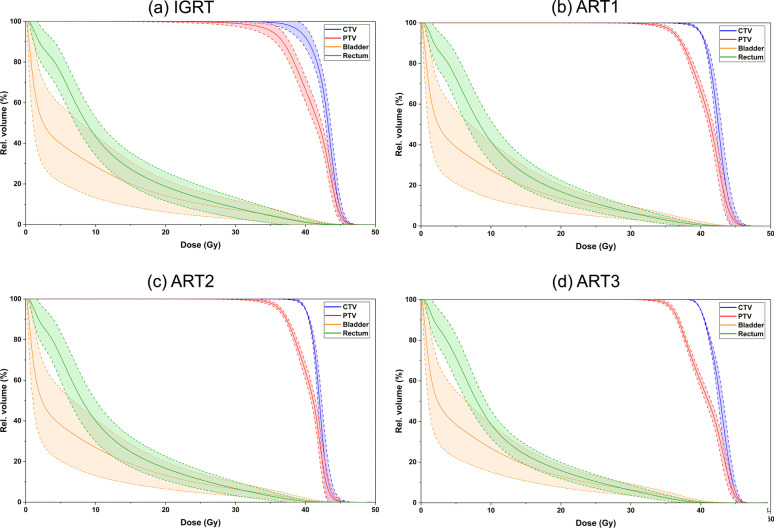
Treatments plans for 32 patients were retrospectively generated and analyzed according to the PACE-C trial treatment scheme (40 Gy in 5 fractions). Using a previously trained cycle-generative adversarial network algorithm, synthetic CT (sCT) were generated out of five daily cone-beam CT. Dose calculation on sCT was performed for four different adaptation approaches: IGRT without adaptation, adaptation via segment aperture morphing (SAM) and segment weight optimization (ART1) or additional shape optimization (ART2) as well as a full re-optimization (ART3). Dose distributions were evaluated regarding dose-volume parameters and a penalty score.
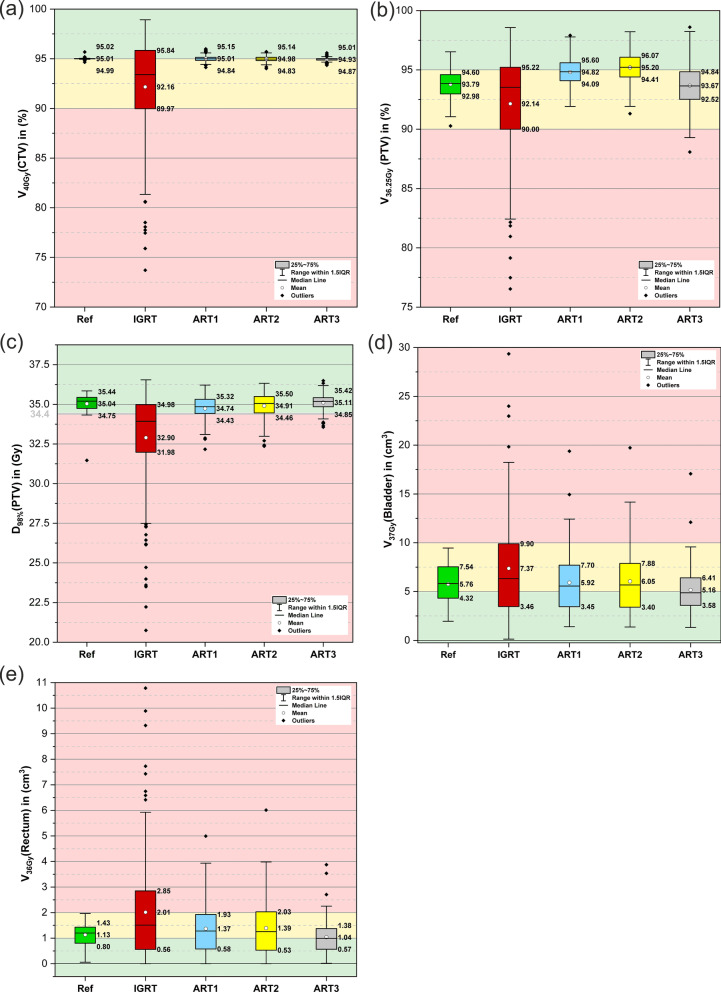
Compared to the IGRT approach, the ART1, ART2 and ART3 approaches substantially reduced the V(bladder) and V(rectum) from a mean of 7.4cm and 2.0cm to (5.9cm, 6.1cm, 5.2cm) as well as to (1.4cm, 1.4cm, 1.0cm), respectively. Plan adaptation required on average 2.6 min for the ART1 approach and yielded doses to the rectum being insignificantly different from the ART2 approach. Based on an accumulation over the total patient collective, a penalty score revealed dosimetric violations reduced by 79.2%, 75.7% and 93.2% through adaptation.
Treatment plan adaptation was demonstrated to adequately restore relevant dose criteria on a daily basis. While for SAM adaptation approaches dosimetric benefits were realized through ensuring sufficient target coverage, a full re-optimization mainly improved OAR sparing which helps to guide the decision of when to apply which adaptation strategy.
在前列腺癌的放射治疗中,越来越多地应用了少分次放疗,这比传统的图像引导放疗(IGRT)对日常治疗的精度要求更高。本研究评估了不同的自适应放疗(ART)策略的剂量学优势。
回顾性地根据 PACE-C 试验治疗方案(40Gy 分 5 次)生成并分析了 32 例患者的治疗计划。使用先前训练的循环生成对抗网络算法,从五次每日锥形束 CT 中生成了合成 CT(sCT)。对 sCT 进行了四种不同适应方法的剂量计算:无适应的 IGRT、通过节段孔径变形(SAM)和节段权重优化(ART1)或附加形状优化(ART2)以及完全重新优化(ART3)的适应。根据剂量-体积参数和惩罚评分评估剂量分布。
与 IGRT 方法相比,ART1、ART2 和 ART3 方法显著降低了膀胱 V(bladder)和直肠 V(rectum)的体积,从平均 7.4cm 和 2.0cm 降至(5.9cm,6.1cm,5.2cm)和(1.4cm,1.4cm,1.0cm)。平均而言,ART1 方法的计划适应需要 2.6 分钟,且直肠剂量与 ART2 方法无显著差异。基于对总患者群体的积累,惩罚评分显示,通过适应,剂量学违规减少了 79.2%、75.7%和 93.2%。
每天治疗时,治疗计划的适应性能够充分恢复相关的剂量标准。虽然 SAM 适应方法通过确保足够的靶区覆盖来实现剂量学优势,但完全重新优化主要改善了 OAR 保护,有助于指导何时应用哪种适应策略。