Jawad Issrah, Rashan Sumayyah, Sigera Chathurani, Salluh Jorge, Dondorp Arjen M, Haniffa Rashan, Beane Abi
National Intensive Care Surveillance-MORU, Borella, Colombo, Western Province, 08, Sri Lanka.
Department of Critical Care and Graduate Program in Translational Medicine, D'Or Institute for Research and Education, Rio de Janeiro, Brazil.
J Intensive Care. 2021 Aug 5;9(1):48. doi: 10.1186/s40560-021-00556-6.
Excess morbidity and mortality following critical illness is increasingly attributed to potentially avoidable complications occurring as a result of complex ICU management (Berenholtz et al., J Crit Care 17:1-2, 2002; De Vos et al., J Crit Care 22:267-74, 2007; Zimmerman J Crit Care 1:12-5, 2002). Routine measurement of quality indicators (QIs) through an Electronic Health Record (EHR) or registries are increasingly used to benchmark care and evaluate improvement interventions. However, existing indicators of quality for intensive care are derived almost exclusively from relatively narrow subsets of ICU patients from high-income healthcare systems. The aim of this scoping review is to systematically review the literature on QIs for evaluating critical care, identify QIs, map their definitions, evidence base, and describe the variances in measurement, and both the reported advantages and challenges of implementation.
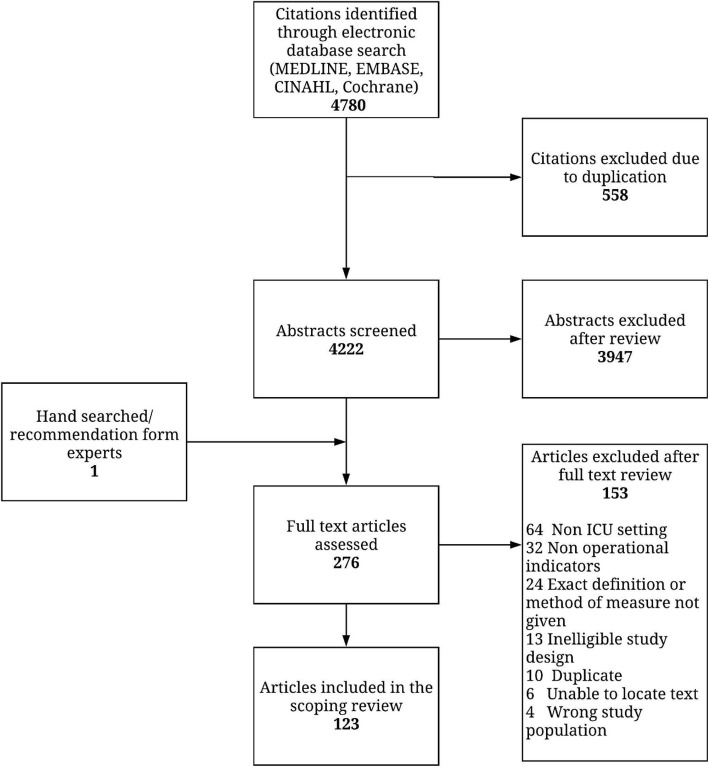
We searched MEDLINE, EMBASE, CINAHL, and the Cochrane libraries from the earliest available date through to January 2019. To increase the sensitivity of the search, grey literature and reference lists were reviewed. Minimum inclusion criteria were a description of one or more QIs designed to evaluate care for patients in ICU captured through a registry platform or EHR adapted for quality of care surveillance.
The search identified 4780 citations. Review of abstracts led to retrieval of 276 full-text articles, of which 123 articles were accepted. Fifty-one unique QIs in ICU were classified using the three components of health care quality proposed by the High Quality Health Systems (HQSS) framework. Adverse events including hospital acquired infections (13.7%), hospital processes (54.9%), and outcomes (31.4%) were the most common QIs identified. Patient reported outcome QIs accounted for less than 6%. Barriers to the implementation of QIs were described in 35.7% of articles and divided into operational barriers (51%) and acceptability barriers (49%).
Despite the complexity and risk associated with ICU care, there are only a small number of operational indicators used. Future selection of QIs would benefit from a stakeholder-driven approach, whereby the values of patients and communities and the priorities for actionable improvement as perceived by healthcare providers are prioritized and include greater focus on measuring discriminable processes of care.
危重症后过高的发病率和死亡率越来越多地归因于复杂的重症监护病房(ICU)管理导致的潜在可避免并发症(贝伦霍尔茨等人,《危重症护理杂志》17:1 - 2,2002年;德沃斯等人,《危重症护理杂志》22:267 - 74,2007年;齐默尔曼,《危重症护理杂志》1:12 - 5,2002年)。通过电子健康记录(EHR)或登记处对质量指标(QIs)进行常规测量越来越多地用于衡量医疗质量和评估改进干预措施。然而,现有的重症监护质量指标几乎完全来自高收入医疗系统中ICU患者相对狭窄的子集。本范围综述的目的是系统回顾关于评估重症监护的质量指标的文献,识别质量指标,梳理其定义、证据基础,描述测量差异以及报告的实施优势和挑战。
我们检索了MEDLINE、EMBASE、CINAHL和Cochrane图书馆,检索时间从各数据库最早收录日期至2019年1月。为提高检索的敏感性,对灰色文献和参考文献列表进行了审查。最低纳入标准是描述一个或多个旨在通过登记平台或适用于医疗质量监测的电子健康记录评估ICU患者护理的质量指标。
检索到4780条引用文献。对摘要的审查导致检索到276篇全文文章,其中123篇文章被接受。使用高质量卫生系统(HQSS)框架提出的医疗质量的三个组成部分对ICU中的51个独特质量指标进行了分类。最常见的质量指标是不良事件,包括医院获得性感染(13.7%)、医院流程(54.9%)和结果(31.4%)。患者报告的结局质量指标占比不到6%。35.7%的文章描述了质量指标实施的障碍,分为操作障碍(51%)和可接受性障碍(49%)。
尽管ICU护理存在复杂性和风险,但使用的操作指标数量很少。未来质量指标的选择将受益于利益相关者驱动的方法,即优先考虑患者和社区的价值观以及医疗服务提供者认为的可采取行动改进的优先事项,并更加注重衡量可区分的护理过程。