Chennai Critical Care Consultants, Pvt Ltd, Chennai, India.
Intensive Care Med. 2022 Nov;48(11):1551-1562. doi: 10.1007/s00134-022-06818-7. Epub 2022 Sep 16.
To develop a set of actionable quality indicators for critical care suitable for use in low- or middle-income countries (LMICs).
A list of 84 candidate indicators compiled from a previous literature review and stakeholder recommendations were categorised into three domains (foundation, process, and quality impact). An expert panel (EP) representing stakeholders from critical care and allied specialties in multiple low-, middle-, and high-income countries was convened. In rounds one and two of the Delphi exercise, the EP appraised (Likert scale 1-5) each indicator for validity, feasibility; in round three sensitivity to change, and reliability were additionally appraised. Potential barriers and facilitators to implementation of the quality indicators were also reported in this round. Median score and interquartile range (IQR) were used to determine consensus; indicators with consensus disagreement (median < 4, IQR ≤ 1) were removed, and indicators with consensus agreement (median ≥ 4, IQR ≤ 1) or no consensus were retained. In round four, indicators were prioritised based on their ability to impact cost of care to the provider and recipient, staff well-being, patient safety, and patient-centred outcomes.
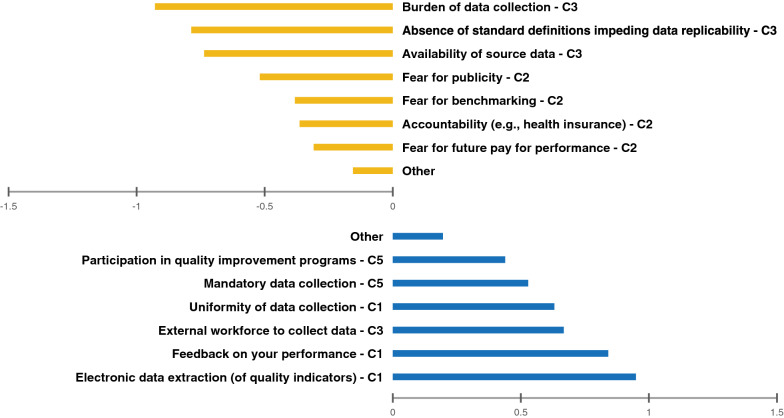
Seventy-one experts from 30 countries (n = 45, 63%, representing critical care) selected 57 indicators to assess quality of care in intensive care unit (ICU) in LMICs: 16 foundation, 27 process, and 14 quality impact indicators after round three. Round 4 resulted in 14 prioritised indicators. Fifty-seven respondents reported barriers and facilitators, of which electronic registry-embedded data collection was the biggest perceived facilitator to implementation (n = 54/57, 95%) Concerns over burden of data collection (n = 53/57, 93%) and variations in definition (n = 45/57, 79%) were perceived as the greatest barrier to implementation.
This consensus exercise provides a common set of indicators to support benchmarking and quality improvement programs for critical care populations in LMICs.
为重症监护制定一套适合中低收入国家(LMICs)使用的可行质量指标。
从先前的文献回顾和利益相关者建议中编制了 84 项候选指标清单,并将其分为三个领域(基础、过程和质量影响)。一个代表来自多个低、中、高收入国家的重症监护和相关专业的利益相关者的专家小组(EP)被召集在一起。在德尔菲法练习的第一和第二轮中,EP 对每个指标的有效性和可行性进行了评估(李克特量表 1-5);在第三轮中,还评估了对变化的敏感性和可靠性。在这一轮中,还报告了实施质量指标的潜在障碍和促进因素。中位数评分和四分位距(IQR)用于确定共识;具有共识分歧的指标(中位数<4,IQR≤1)被删除,具有共识一致的指标(中位数≥4,IQR≤1)或没有共识的指标被保留。在第四轮中,根据对提供者和接受者的护理成本、员工福祉、患者安全和以患者为中心的结果的影响能力对指标进行了优先级排序。
来自 30 个国家的 71 名专家(n=45,63%,代表重症监护)选择了 57 项指标来评估中低收入国家重症监护病房(ICU)的护理质量:经过三轮后,有 16 项基础指标、27 项过程指标和 14 项质量影响指标。第四轮产生了 14 项优先指标。57 名受访者报告了障碍和促进因素,其中电子登记嵌入数据收集被认为是实施的最大促进因素(n=54/57,95%)。对数据收集负担的担忧(n=53/57,93%)和定义的差异(n=45/57,79%)被认为是实施的最大障碍。
这项共识性工作为中低收入国家重症监护人群的基准测试和质量改进计划提供了一套共同的指标。