Schmitz Lilith, Hoermann Pamela, Trutnau Birgit, Jankauskiene Augustina, Zaloszyc Ariane, Edefonti Alberto Carlo, Schmitt Claus Peter, Klaus Guenter
Department of Pediatric Nephrology, University of Marburg, Marburg, Germany.
KfH Pediatric Kidney Center and University Hospital, University of Marburg, Marburg, Germany.
Front Pediatr. 2021 Jul 20;9:666101. doi: 10.3389/fped.2021.666101. eCollection 2021.
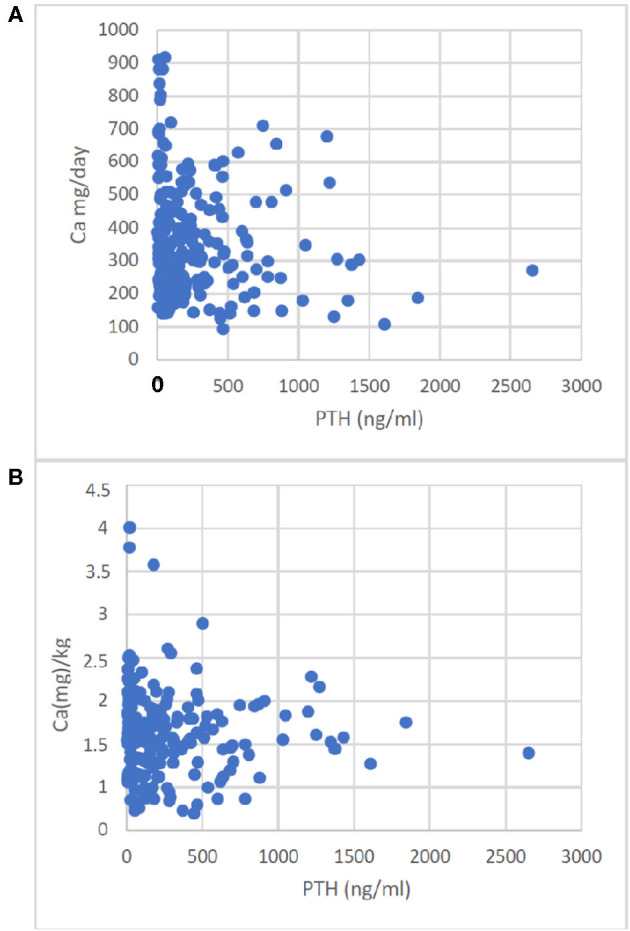
Treatment of chronic kidney disease (CKD) mineral bone disorder (MBD) is challenging in growing children due to the high amount of calcium needed for normal bone mineralization and the required dietary phosphate restriction, which often includes intake of calcium-rich products such as milk. Therefore, enteral calcium-intake (Ca-I) was calculated. We looked at pediatric CKD-Patients aged 0-6 years. We used a retrospective analysis of Ca-I from dietary data collections. Ca-I below 60% or above 100% of the D-A-CH and the KDOQI reference values were considered as severe Ca deficiency or Ca overload, respectively. We had 41 children, median age 1.1 (range 0-5.8) years, body weight 7.3 (2.4-19.9) kg, and length 68 (48-105) cm at the time of first dietary data collection. Renal function was classified as CKD stage III in 20, IV in 28, V in 44, and VD in 142 dietary data collections. At the first dietary data collection, 5 children were in the CKD stage III, 10 in IV, 9 in V, and 17 were on dialysis. Only one child progressed to a higher CKD stage. In total, 234 dietary data collections were analyzed, and 65 follow-up collections were available from 33 children after a time interval of 26 (1-372) days. The median caloric intake was 120 (47-217)% of D-A-CH RDI. In 149 (63.6%) of the dietary data collections, enteral Ca-I was below the target (<100% of the D-A-CH and KDOQI RDI). Severe Ca-deficiency was found in 11 (26%) and 4 (12%) of the children at the first and second dietary data collection, respectively. In total, 11 children were on Ca-containing phosphate binders. In dietary data collection 1 and 2, there were seven children. From these, 4/7 and 4/7 patients had an enteral total Ca-I above the 100% D-A-CH-limit or above the KDOQI limit, respectively. Absolute dietary Ca-I and Ca-I normalized to body weight correlated negatively with PTH (r = -0.196, < 0.005 and r = -0.13, < 0.05). Enteral Ca-I should repeatedly be monitored in CKD children because many may may otherwise be underexposed to enteral calcium and overexposed when calcium-containing phosphate binders are given. Our findings suggest a major impact of dietary calcium supply on bone health in pediatric CKD.
由于正常骨矿化需要大量钙,且饮食中需要限制磷的摄入(这通常包括摄入富含钙的产品,如牛奶),因此,治疗生长中儿童的慢性肾脏病(CKD)矿物质骨病(MBD)具有挑战性。因此,我们计算了肠道钙摄入量(Ca-I)。我们研究了0至6岁的儿科CKD患者。我们对饮食数据收集的Ca-I进行了回顾性分析。低于D-A-CH和KDOQI参考值60%或高于100%的Ca-I分别被视为严重钙缺乏或钙过载。在首次饮食数据收集时,我们有41名儿童,中位年龄1.1(范围0-5.8)岁,体重7.3(2.4-19.9)kg,身长68(48-105)cm。在20次、28次、44次和142次饮食数据收集中,肾功能分别被分类为CKD 3期、4期、5期和5D期。在首次饮食数据收集时,5名儿童处于CKD 3期,10名处于4期,9名处于5期,17名正在接受透析。只有一名儿童进展到更高的CKD阶段。总共分析了234次饮食数据收集,在26(1-372)天的时间间隔后,从33名儿童中获得了65次随访收集。中位热量摄入为D-A-CH推荐膳食摄入量(RDI)的120(47-217)%。在149(63.6%)次饮食数据收集中,肠道Ca-I低于目标值(<D-A-CH和KDOQI RDI的100%)。在首次和第二次饮食数据收集时,分别有11(26%)名和4(12%)名儿童被发现严重缺钙。总共有11名儿童服用含钙磷结合剂。在饮食数据收集1和2中,有7名儿童。其中,分别有4/7和4/7的患者肠道总Ca-I高于100%D-A-CH限值或高于KDOQI限值。绝对饮食Ca-I和按体重标准化的Ca-I与甲状旁腺激素(PTH)呈负相关(r = -0.196,<0.005和r = -0.13,<0.05)。应反复监测CKD儿童的肠道Ca-I,因为否则许多儿童可能肠道钙摄入不足,而在给予含钙磷结合剂时则会摄入过量。我们的研究结果表明,饮食钙供应对儿科CKD患者的骨骼健康有重大影响。