Center for Pediatrics and Adolescent Medicine, Heidelberg, Germany.
Institute of Medical Biometry and Informatics, University of Heidelberg, Heidelberg, Germany.
Sci Rep. 2019 Mar 20;9(1):4886. doi: 10.1038/s41598-018-36975-z.
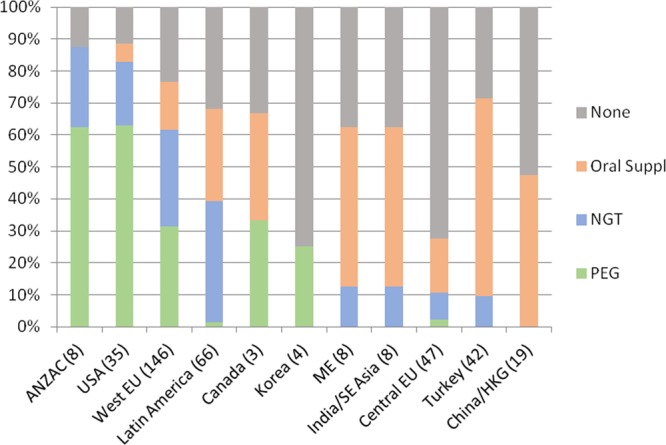
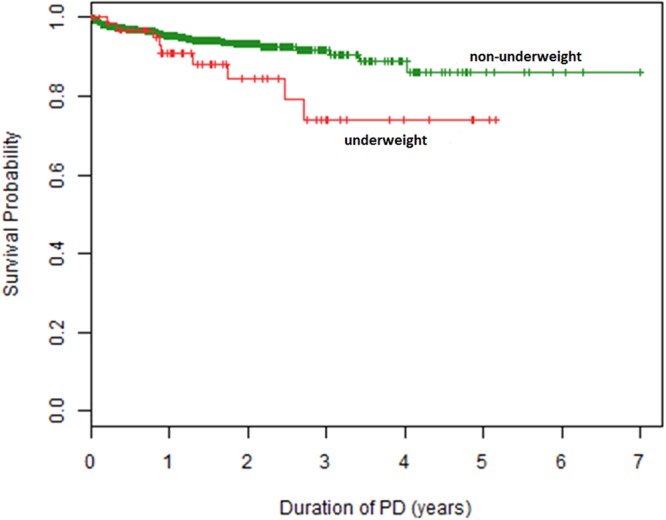
While children approaching end-stage kidney disease (ESKD) are considered at risk of uremic anorexia and underweight they are also exposed to the global obesity epidemic. We sought to investigate the variation of nutritional status in children undergoing chronic peritoneal dialysis (CPD) around the globe. The distribution and course of body mass index (BMI) standard deviation score over time was examined prospectively in 1001 children and adolescents from 35 countries starting CPD who were followed in the International Pediatric PD Network (IPPN) Registry. The overall prevalence of underweight, and overweight/obesity at start of CPD was 8.9% and 19.7%, respectively. Underweight was most prevalent in South and Southeast Asia (20%), Central Europe (16.7%) and Turkey (15.2%), whereas overweight and obesity were most common in the Middle East (40%) and the US (33%). BMI SDS at PD initiation was associated positively with current eGFR and gastrostomy feeding prior to PD start. Over the course of PD BMI SDS tended to increase on CPD in underweight and normal weight children, whereas it decreased in initially overweight patients. In infancy, mortality risk was amplified by obesity, whereas in older children mortality was markedly increased in association with underweight. Both underweight and overweight are prevalent in pediatric ESKD, with the prevalence varying across the globe. Late dialysis start is associated with underweight, while enteral feeding can lead to obesity. Nutritional abnormalities tend to attenuate with time on dialysis. Mortality risk appears increased with obesity in infants and with underweight in older children.
虽然接近终末期肾病 (ESKD) 的儿童被认为存在尿毒症性厌食和体重不足的风险,但他们也面临着全球肥胖症的流行。我们试图研究全球范围内接受慢性腹膜透析 (CPD) 的儿童的营养状况变化。在国际儿科 PD 网络 (IPPN) 注册中心,前瞻性地对来自 35 个国家的 1001 名开始 CPD 的儿童和青少年进行了研究,观察他们的体重指数 (BMI) 标准差评分随时间的分布和变化过程。开始 CPD 时,体重不足和超重/肥胖的总体患病率分别为 8.9%和 19.7%。体重不足在南亚和东南亚(20%)、中欧(16.7%)和土耳其(15.2%)最为常见,而超重和肥胖在中东(40%)和美国(33%)最为常见。PD 起始时的 BMI SDS 与当前 eGFR 和 PD 起始前的胃造口喂养呈正相关。在接受 CPD 的过程中,BMI SDS 在体重不足和正常体重的儿童中趋于增加,而在最初超重的患者中则降低。在婴儿期,肥胖会放大死亡风险,而在较大的儿童中,与体重不足相关的死亡风险显著增加。在儿科 ESKD 中,体重不足和超重都很常见,其患病率在全球范围内存在差异。晚期透析开始与体重不足有关,而肠内喂养可能导致肥胖。随着透析时间的延长,营养异常往往会减轻。肥胖会增加婴儿的死亡风险,而体重不足会增加较大儿童的死亡风险。