Kwong Allison J, Ghaziani T Tara, Yao Francis, Sze Daniel, Mannalithara Ajitha, Mehta Neil
Division of Gastroenterology and Hepatology, Stanford, California.
Division of Gastroenterology, University of California, San Francisco, San Francisco, California.
Clin Gastroenterol Hepatol. 2022 May;20(5):1142-1150.e4. doi: 10.1016/j.cgh.2021.07.048. Epub 2021 Aug 3.
BACKGROUND & AIMS: Policy changes in the United States have lengthened overall waiting times for patients with hepatocellular carcinoma (HCC). We investigated temporal trends in utilization of locoregional therapy (LRT) and associated waitlist outcomes among liver transplant (LT) candidates in the United States.
Data for primary adult LT candidates listed from 2003 to 2018 who received HCC exception were extracted from the Organ Procurement and Transplantation Network database. Explant histology was examined, and multivariable competing risk analysis was used to evaluate the association between LRT type and waitlist dropout.
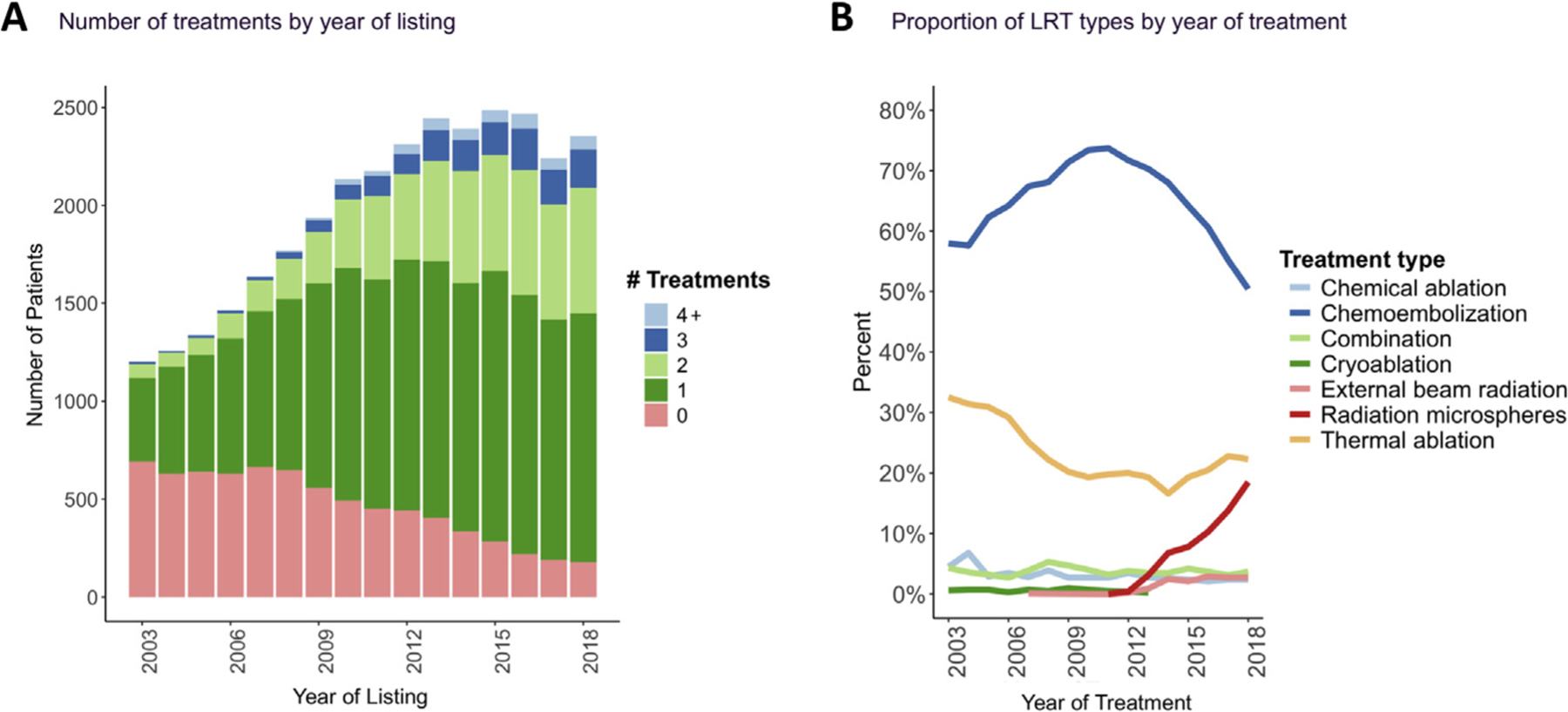
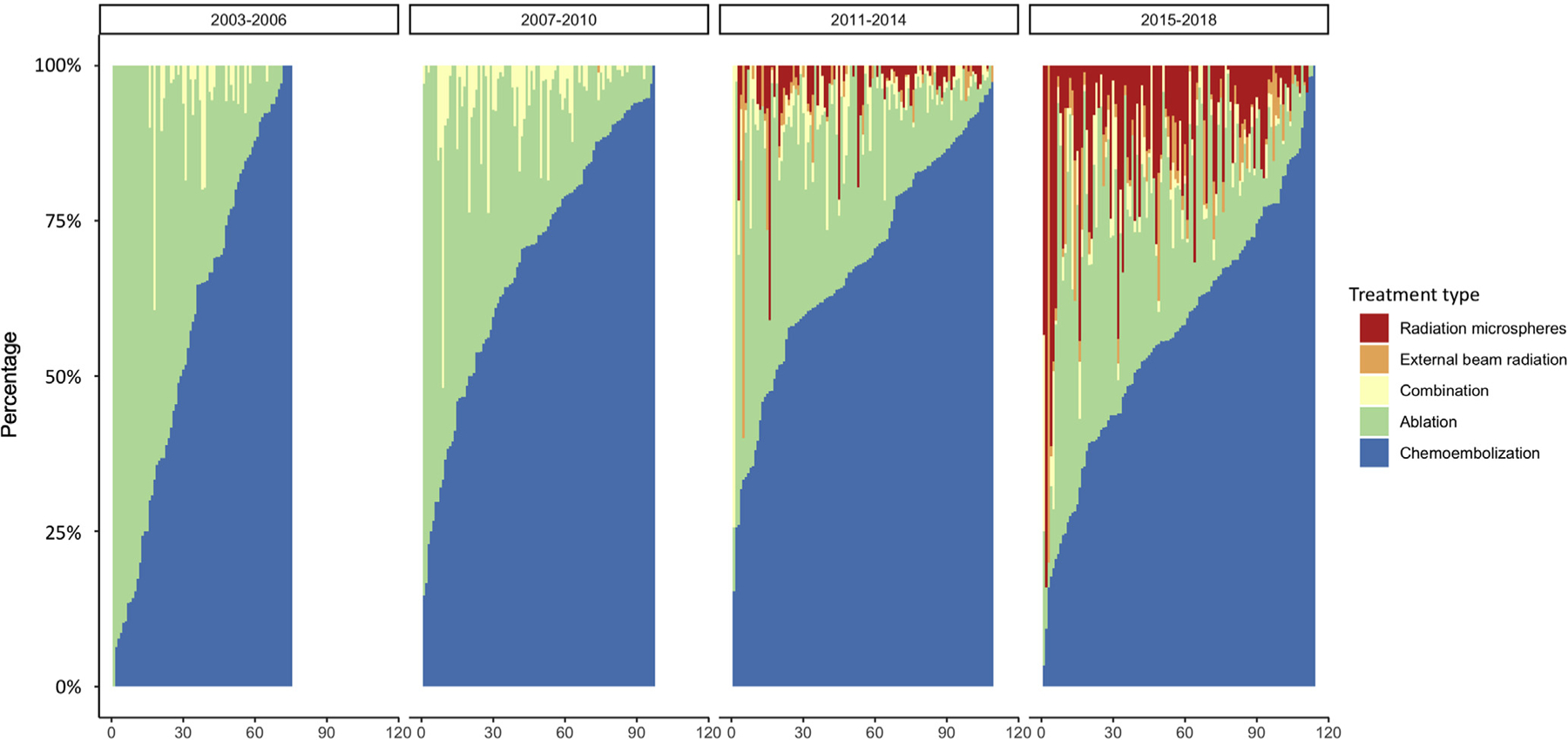
There were 31,609 eligible patients with at least 1 approved HCC exception, and 34,610 treatments among 24,145 LT candidates. The proportion with at least 1 LRT recorded increased from 42.3% in 2003 to 92.4% in 2018. Chemoembolization remains the most frequent type, followed by thermal ablation, with a notable increase in radioembolization from 3% in 2013 to 19% in 2018. An increased incidence of LRT was observed among patients with tumor burden beyond Milan criteria, higher α-fetoprotein level, and more compensated liver disease. Receipt of any type of LRT was associated with a lower risk of waitlist dropout; there was no significant difference by number of LRTs. In inverse probability of treatment weighting-adjusted analysis, radioembolization or ablation as the first LRT was associated with a reduced risk of waitlist dropout compared with chemoembolization.
In a large nationwide cohort of LT candidates with HCC, LRT, and in particular radioembolization, increasingly was used to bridge to LT. Patients with greater tumor burden and those with more compensated liver disease received more treatments while awaiting LT. Bridging LRT was associated with a lower risk of waitlist dropout.
美国的政策变化延长了肝细胞癌(HCC)患者的总体等待时间。我们调查了美国肝移植(LT)候选者局部区域治疗(LRT)的使用时间趋势及相关等待名单结果。
从器官获取与移植网络数据库中提取2003年至2018年列出的接受HCC例外的原发性成年LT候选者的数据。检查切除组织学,并使用多变量竞争风险分析来评估LRT类型与等待名单退出之间的关联。
有31609名符合条件的患者至少有1次批准的HCC例外,24145名LT候选者中有34610次治疗。记录到至少接受1次LRT的比例从2003年的42.3%增加到2018年的92.4%。化疗栓塞仍然是最常见的类型,其次是热消融,放射性栓塞从2013年的3%显著增加到2018年的19%。在肿瘤负担超过米兰标准、甲胎蛋白水平较高和肝病代偿较好的患者中观察到LRT发生率增加。接受任何类型的LRT与等待名单退出风险较低相关;LRT的次数没有显著差异。在治疗权重逆概率调整分析中,与化疗栓塞相比,放射性栓塞或消融作为首次LRT与等待名单退出风险降低相关。
在一个全国性的大型HCC、LRT的LT候选者队列中,尤其是放射性栓塞,越来越多地用于过渡到LT。肿瘤负担较大和肝病代偿较好的患者在等待LT期间接受了更多的治疗。过渡性LRT与等待名单退出风险较低相关。