Department of internal Medicine, Division of Endocrinology, Erasmus Medical Center, 40, 3015 GD Rotterdam, The Netherlands.
Int J Mol Sci. 2021 Jul 21;22(15):7797. doi: 10.3390/ijms22157797.
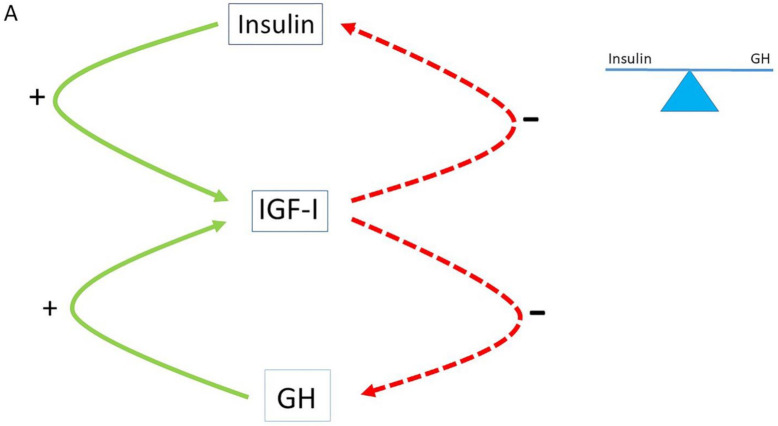
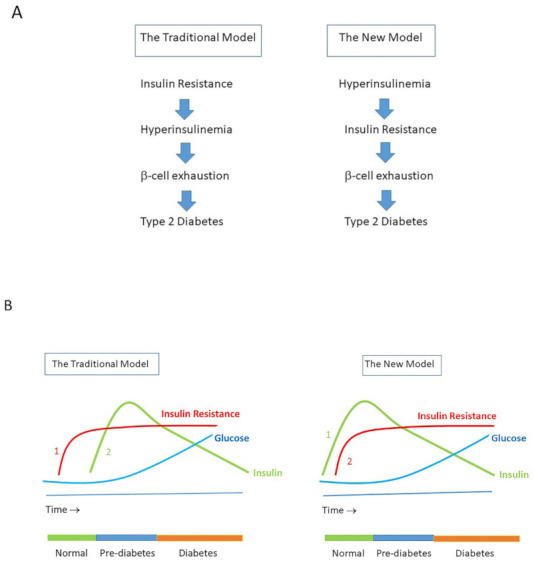
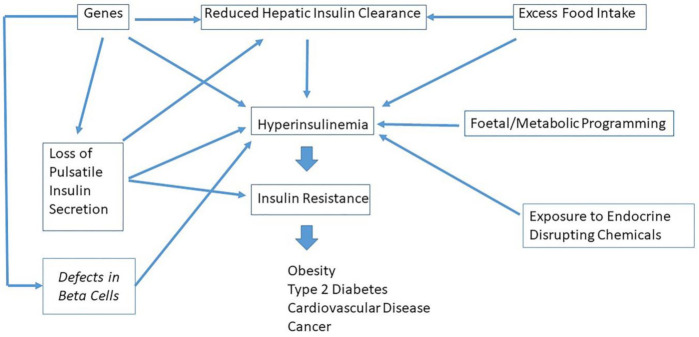
For many years, the dogma has been that insulin resistance precedes the development of hyperinsulinemia. However, recent data suggest a reverse order and place hyperinsulinemia mechanistically upstream of insulin resistance. Genetic background, consumption of the "modern" Western diet and over-nutrition may increase insulin secretion, decrease insulin pulses and/or reduce hepatic insulin clearance, thereby causing hyperinsulinemia. Hyperinsulinemia disturbs the balance of the insulin-GH-IGF axis and shifts the insulin : GH ratio towards insulin and away from GH. This insulin-GH shift promotes energy storage and lipid synthesis and hinders lipid breakdown, resulting in obesity due to higher fat accumulation and lower energy expenditure. Hyperinsulinemia is an important etiological factor in the development of metabolic syndrome, type 2 diabetes, cardiovascular disease, cancer and premature mortality. It has been further hypothesized that nutritionally driven insulin exposure controls the rate of mammalian aging. Interventions that normalize/reduce plasma insulin concentrations might play a key role in the prevention and treatment of age-related decline, obesity, type 2 diabetes, cardiovascular disease and cancer. Caloric restriction, increasing hepatic insulin clearance and maximizing insulin sensitivity are at present the three main strategies available for managing hyperinsulinemia. This may slow down age-related physiological decline and prevent age-related diseases. Drugs that reduce insulin (hyper) secretion, normalize pulsatile insulin secretion and/or increase hepatic insulin clearance may also have the potential to prevent or delay the progression of hyperinsulinemia-mediated diseases. Future research should focus on new strategies to minimize hyperinsulinemia at an early stage, aiming at successfully preventing and treating hyperinsulinemia-mediated diseases.
多年来,一直存在这样一种教条,即胰岛素抵抗先于高胰岛素血症的发生。然而,最近的数据表明,这种关系可能相反,高胰岛素血症在机制上先于胰岛素抵抗发生。遗传背景、“现代”西方饮食的摄入和营养过剩可能会增加胰岛素分泌、减少胰岛素脉冲和/或降低肝脏胰岛素清除率,从而导致高胰岛素血症。高胰岛素血症扰乱了胰岛素-GH-IGF 轴的平衡,使胰岛素:GH 比值向胰岛素倾斜,远离 GH。这种胰岛素-GH 转移促进能量储存和脂质合成,并阻碍脂质分解,导致脂肪堆积增加和能量消耗减少,从而导致肥胖。高胰岛素血症是代谢综合征、2 型糖尿病、心血管疾病、癌症和早逝发展的重要病因。进一步的假设是,营养驱动的胰岛素暴露控制着哺乳动物衰老的速度。使血浆胰岛素浓度正常化/降低的干预措施可能在预防和治疗与年龄相关的衰退、肥胖、2 型糖尿病、心血管疾病和癌症方面发挥关键作用。热量限制、增加肝脏胰岛素清除率和最大限度地提高胰岛素敏感性是目前用于治疗高胰岛素血症的三种主要策略。这可能会减缓与年龄相关的生理衰退并预防与年龄相关的疾病。降低胰岛素(高)分泌、使胰岛素脉冲分泌正常化和/或增加肝脏胰岛素清除率的药物也可能具有预防或延缓高胰岛素血症介导的疾病进展的潜力。未来的研究应侧重于在早期阶段将高胰岛素血症最小化的新策略,旨在成功预防和治疗高胰岛素血症介导的疾病。