Lusho Sejdi, Durando Xavier, Mouret-Reynier Marie-Ange, Kossai Myriam, Lacrampe Nathalie, Molnar Ioana, Penault-Llorca Frederique, Radosevic-Robin Nina, Abrial Catherine
Clermont Auvergne University, INSERM U1240 "Molecular Imaging and Theranostic Strategies", Centre Jean Perrin, Clermont-Ferrand, France.
Delegation for Clinical Research and Innovation, Centre Jean Perrin, Clermont-Ferrand, France.
Front Oncol. 2021 Jul 20;11:678315. doi: 10.3389/fonc.2021.678315. eCollection 2021.
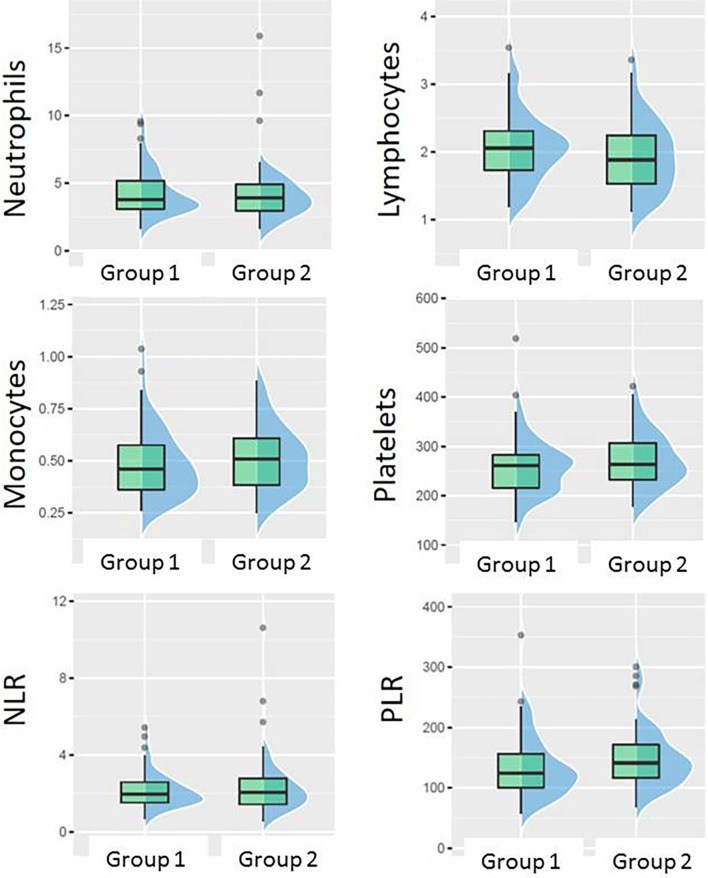
Triple negative breast cancer (TNBC) is highly heterogeneous, but still most of the patients are treated by the anthracycline/taxane-based neoadjuvant therapy (NACT). Tumor-infiltrating lymphocytes (TILs) are a strong predictive and prognostic biomarker in TNBC, however are not always available. Peripheral blood counts, which reflect the systemic inflammatory/immune status, are easier to obtain than TILs. We investigated whether baseline white cell or platelet counts, as well as, Neutrophil-to-Lymphocyte Ratio (NLR) or Platelet-to-Lymphocyte Ratio (PLR) could replace baseline TILs as predictive or prognostic biomarkers in a series of TNBC treated by standard NACT.
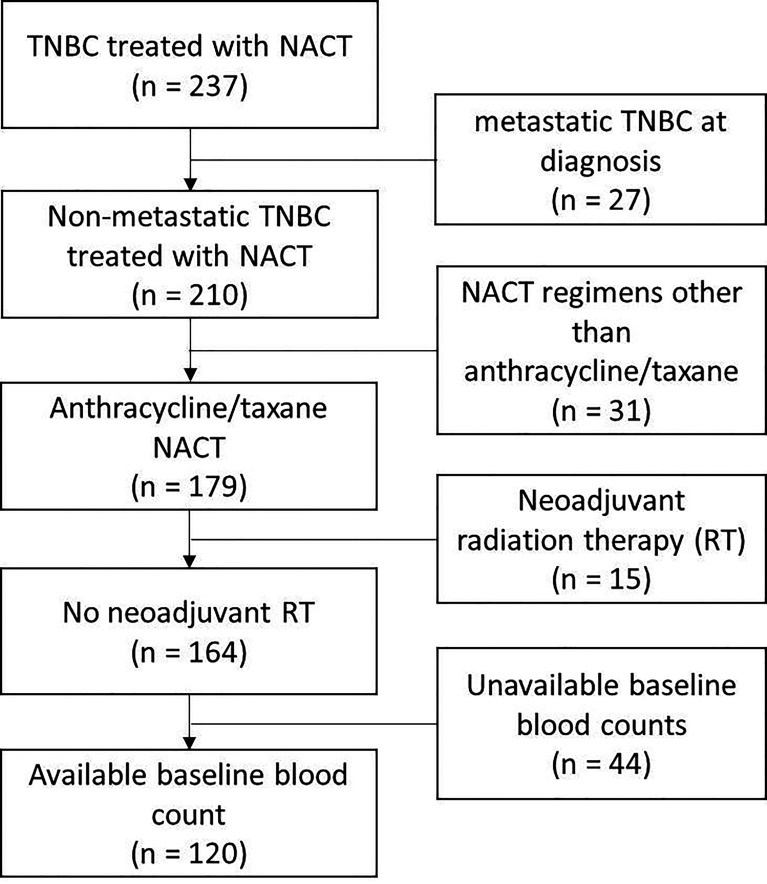
One hundred twenty patients uniformly treated by FEC/taxane NACT in a tertiary cancer care center were retrospectively analyzed. The presence of pathological complete response (pCR: ypT0/Tis, ypN0) or the presence of pCR and/small residual disease (ypT0/Tis/T1ab, ypN0) were considered as good responses in data analysis. Baseline/pre-NACT blood count, NLR, PLR and TILs were evaluated as predictors of response, distant recurrence rate and distant recurrence-free survival (DRFS).
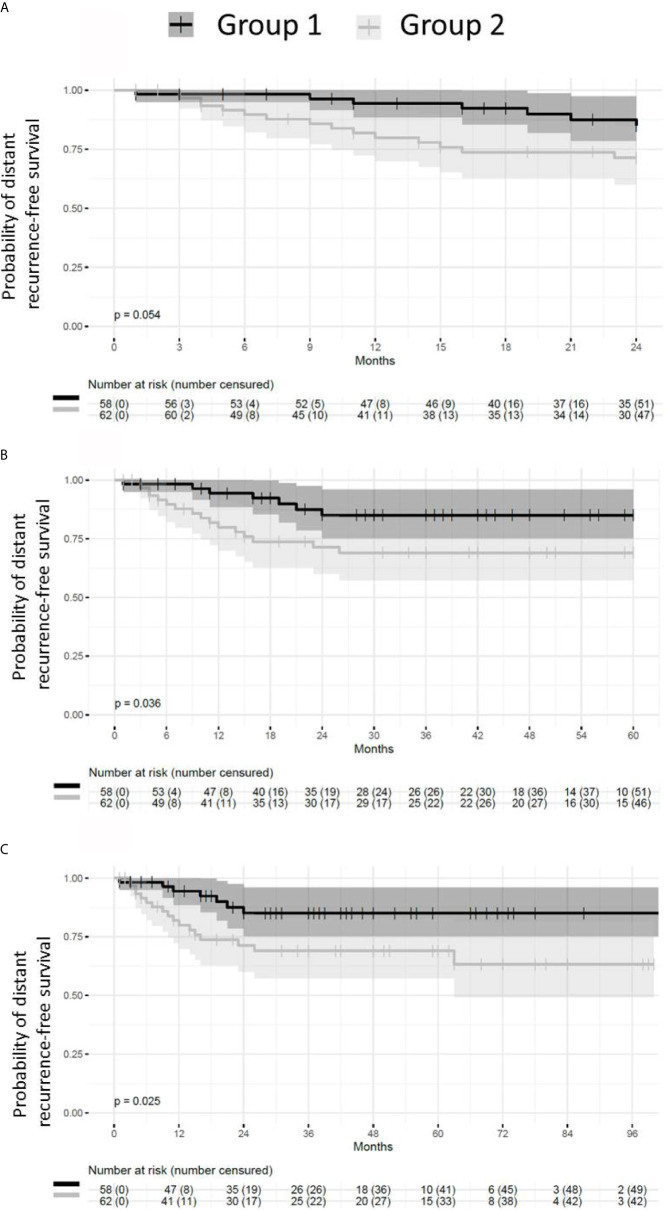
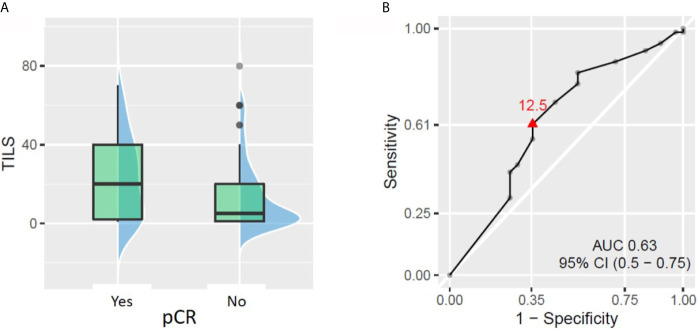
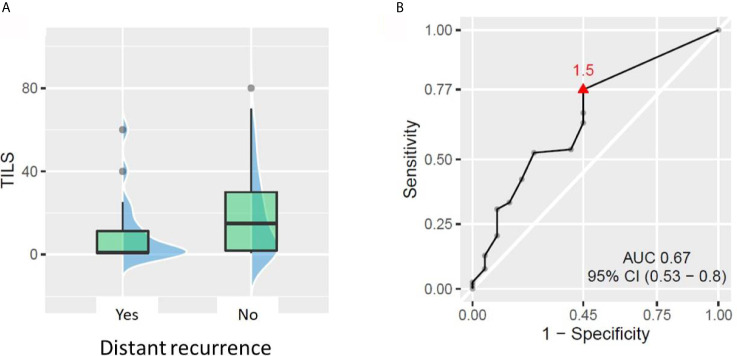
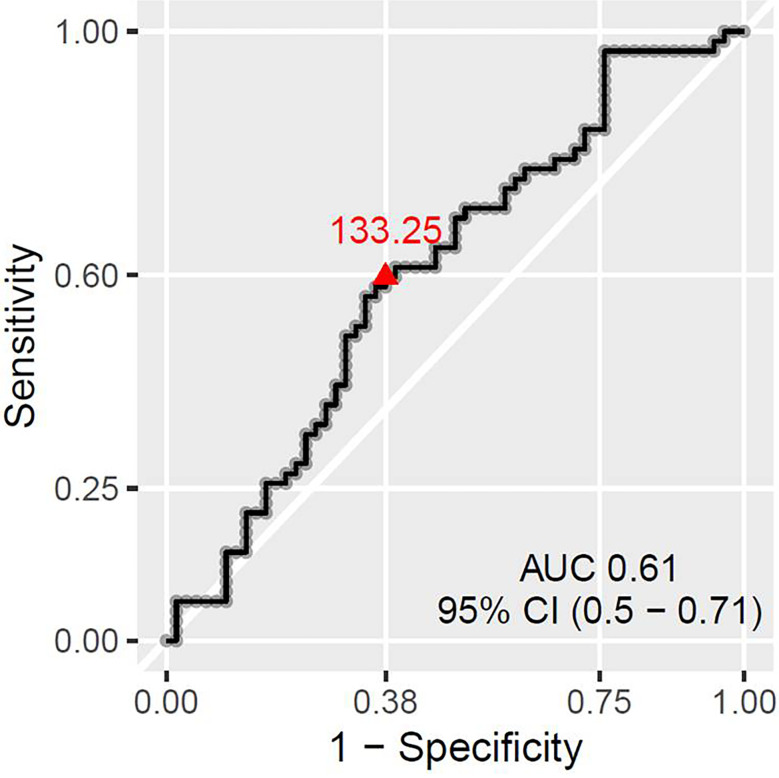
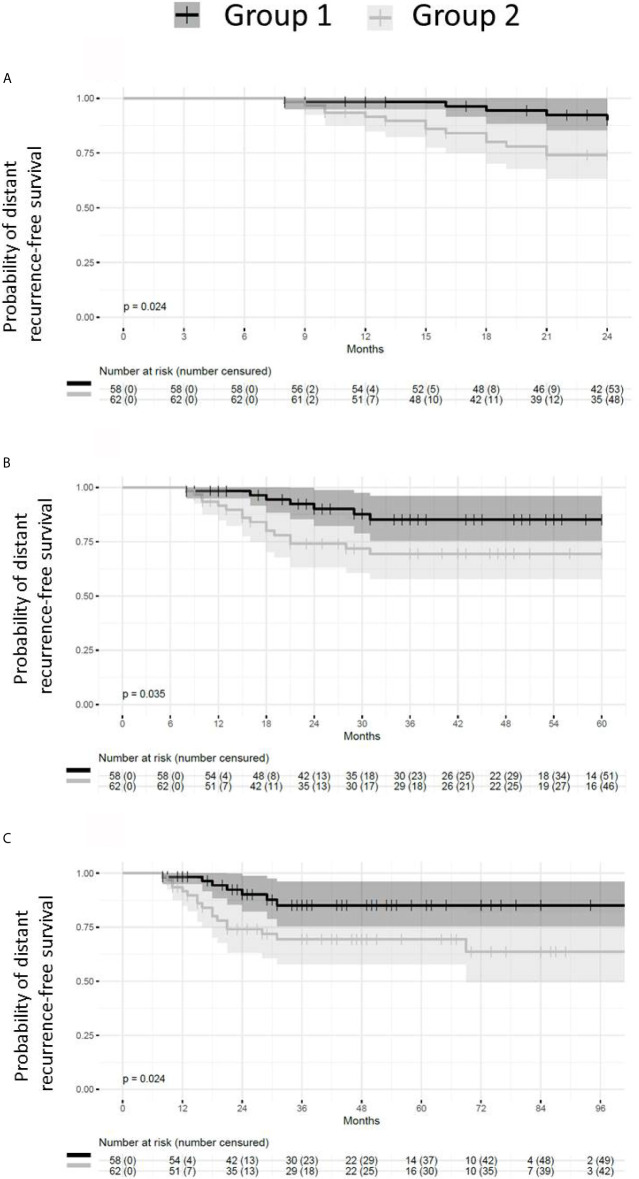
TILs ≥30% and ≥1.5% were best predictors of pCR and distant recurrence risk, respectively (p = 0.007, p = 0.012). However, in this cohort, pCR status was not significantly associated with recurrence. Only the ensemble of patients with pCR and small residual disease had lower recurrence risk and longer survival DRFS (p = 0.042, p = 0.024, respectively) than the rest of the cohort (larger residual disease). The only parameter which could predict the pCR/small residual disease status was PLR: patients with values lower than 133.25 had significantly higher chance of reaching that status after NACT (p = 0.045). However, no direct correlation could be established between baseline PLR and metastatic recurrence. No correlation either was found between TIL and individual blood counts, or between TILs and NLR or PLR.
In this cohort, TILs retained their pCR predictive value; however PLR was a better predictor of the ensemble of responses which had good outcome in terms of less distant recurrences or longer DRFS (pCR or small residual disease). Thus, baseline PLR is worth further, prospective investigation together with baseline TILs, as it might indicate a good TNBC response to NACT when TILs are unavailable.
三阴性乳腺癌(TNBC)具有高度异质性,但大多数患者仍接受基于蒽环类/紫杉烷的新辅助治疗(NACT)。肿瘤浸润淋巴细胞(TILs)是TNBC中一种强大的预测和预后生物标志物,但并非总是可用。反映全身炎症/免疫状态的外周血细胞计数比TILs更容易获得。我们研究了在一系列接受标准NACT治疗的TNBC患者中,基线白细胞或血小板计数以及中性粒细胞与淋巴细胞比值(NLR)或血小板与淋巴细胞比值(PLR)是否可以替代基线TILs作为预测或预后生物标志物。
回顾性分析了一家三级癌症护理中心120例接受FEC/紫杉烷NACT统一治疗的患者。在数据分析中,病理完全缓解(pCR:ypT0/Tis,ypN0)或pCR和/或小残留疾病(ypT0/Tis/T1ab,ypN0)的存在被视为良好反应。评估基线/新辅助治疗前的血细胞计数、NLR、PLR和TILs作为反应、远处复发率和远处无复发生存期(DRFS)的预测指标。
TILs≥30%和≥1.5%分别是pCR和远处复发风险的最佳预测指标(p = 0.007,p = 0.012)。然而,在该队列中,pCR状态与复发无显著相关性。只有pCR和小残留疾病的患者群体比其余队列(较大残留疾病)具有更低的复发风险和更长的DRFS生存期(分别为p = 0.042,p = 0.024)。唯一能够预测pCR/小残留疾病状态的参数是PLR:值低于133.25的患者在NACT后达到该状态的机会显著更高(p = 0.045)。然而,无法在基线PLR与转移性复发之间建立直接相关性。在TIL与个体血细胞计数之间,或TILs与NLR或PLR之间也未发现相关性。
在该队列中,TILs保留了其pCR预测价值;然而,PLR是对远处复发较少或DRFS较长(pCR或小残留疾病)的良好结局反应群体的更好预测指标。因此,基线PLR值得与基线TILs一起进行进一步的前瞻性研究,因为当TILs不可用时,它可能表明TNBC对NACT有良好反应。