Chongqing Key Laboratory of Human Embryo Engineering, Chongqing, China.
Chongqing Clinical Research Center for Reproductive Medicine, Chongqing, China.
Reprod Biol Endocrinol. 2021 Aug 12;19(1):124. doi: 10.1186/s12958-021-00814-0.
A consensus has been reached on the preferred primary outcome of all infertility treatment trials, which is the cumulative live birth rate (CLBR). Some recent randomized controlled trials (RCTs) and retrospective studies have compared the effectiveness of GnRH-antagonist and GnRH-agonist protocols but showed inconsistent results. Studies commonly used conservative estimates and optimal estimates to described the CLBR of one incomplete assisted reproductive technology (ART) cycle and there are not many previous studies with data of the complete cycle to compare CLBRs in GnRH-antagonist versus GnRH-agonist protocols.
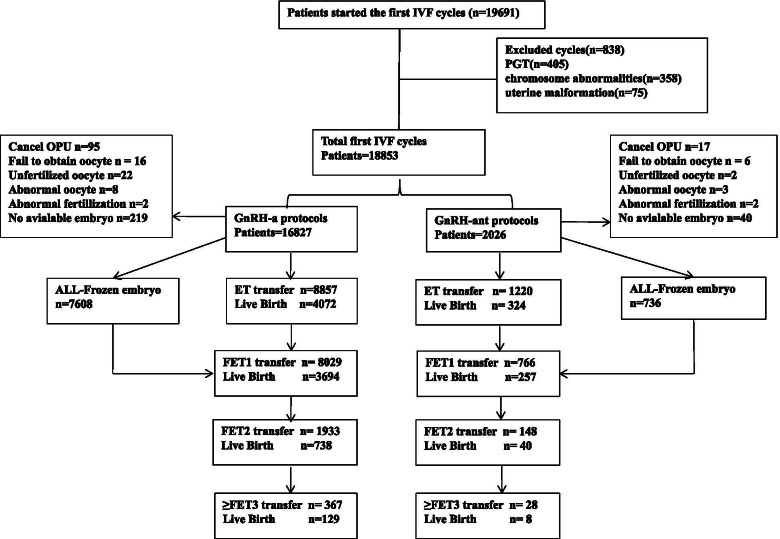
A total of 18,853 patients have completed their first IVF cycle including fresh and subsequent frozen-thawed cycles during 2016-2019, 16,827 patients were treated with GnRH-a long and 2026 patients with GnRH-ant protocol. Multivariable logistic analysis was used to evaluate the difference of GnRH-a and GnRH-ant protocol in relation to CLBR. Utilized Propensity Score Matching(PSM) for sampling by up to 1:1 nearest neighbor matching to adjust the numerical difference and balance the confounders between groups.
Before PSM, significant differences were observed in baseline characteristics and the CLBR was 50.91% in the GnRH-a and 33.42% in the GnRH-ant (OR = 2.07; 95%CI: 1.88-2.28; P < 0.001). Stratified analysis showed the CLBR of GnRH-ant was lower than GnRH-a in suboptimal responders(46.89 vs 27.42%, OR = 2.34, 95%CI = 1.99-2.74; P < 0.001) and no differences of CLBR were observed in other patients between protocols. After adjusting for potential confounders, multivariable logistic analysis found the CLBR of GnRH-ant group was lower than that of GnRH-a group (OR = 2.11, 95%CI:1.69-2.63, P < 0.001). After PSM balenced the confounders between groups, the CLBR of GnRH-a group was higher than that of GnRH-ant group in suboptimal responders((38.61 vs 28.22%, OR = 1.60, 95%CI = 1.28-1.99; P < 0.001) and the normal fertilization rate and number of available embryo in GnRH-a were higher than these of GnRH-ant groups in suboptimal responders (77.39 vs 75.22%; 2.86 ± 1.26 vs 2.61 ± 1.22; P < 0.05). No significant difference was observed in other patients between different protocols.
It is crucial to optimize the utilization of protocols in different ovarian response patients and reconsider the field of application of GnRH-ant protocols in China.
人们已经就所有不孕治疗试验的首选主要结局达成共识,即累积活产率(CLBR)。一些最近的随机对照试验(RCT)和回顾性研究比较了 GnRH 拮抗剂和 GnRH 激动剂方案的有效性,但结果不一致。研究通常使用保守估计和最佳估计来描述一个不完全的辅助生殖技术(ART)周期的 CLBR,并且之前很少有研究有完整周期的数据来比较 GnRH 拮抗剂与 GnRH 激动剂方案的 CLBR。
共有 18853 名患者在 2016-2019 年期间完成了他们的第一次 IVF 周期,包括新鲜和随后的冷冻解冻周期,其中 16827 名患者接受了 GnRH-a 长方案治疗,2026 名患者接受了 GnRH 拮抗剂方案治疗。多变量逻辑分析用于评估 GnRH-a 和 GnRH 拮抗剂方案在 CLBR 方面的差异。利用倾向评分匹配(PSM)进行采样,最多采用 1:1 最近邻匹配来调整组间的数值差异和平衡混杂因素。
在 PSM 之前,基线特征存在显著差异,GnRH-a 组的 CLBR 为 50.91%,GnRH 拮抗剂组为 33.42%(OR=2.07;95%CI:1.88-2.28;P<0.001)。分层分析显示,在反应不佳的患者中,GnRH 拮抗剂组的 CLBR 低于 GnRH-a 组(46.89%比 27.42%,OR=2.34,95%CI=1.99-2.74;P<0.001),而在其他患者中,两种方案之间的 CLBR 无差异。调整潜在混杂因素后,多变量逻辑分析发现 GnRH 拮抗剂组的 CLBR 低于 GnRH-a 组(OR=2.11,95%CI:1.69-2.63,P<0.001)。在 PSM 平衡了组间混杂因素后,在反应不佳的患者中,GnRH-a 组的 CLBR 高于 GnRH 拮抗剂组(38.61%比 28.22%,OR=1.60,95%CI=1.28-1.99;P<0.001),在反应不佳的患者中,GnRH-a 组的正常受精率和可用胚胎数均高于 GnRH 拮抗剂组(77.39%比 75.22%;2.86±1.26 比 2.61±1.22;P<0.05)。在其他患者中,两种方案之间没有显著差异。
在不同卵巢反应患者中优化方案的应用至关重要,并重新考虑 GnRH 拮抗剂方案在中国的应用领域。