Morita-Sherman Marcia, Li Manshi, Joseph Boney, Yasuda Clarissa, Vegh Deborah, De Campos Brunno Machado, Alvim Marina K M, Louis Shreya, Bingaman William, Najm Imad, Jones Stephen, Wang Xiaofeng, Blümcke Ingmar, Brinkmann Benjamin H, Worrell Gregory, Cendes Fernando, Jehi Lara
Department of Neurology, Epilepsy Center, Cleveland Clinic, Cleveland, OH, USA.
Department of Quantitative Health Sciences, Quantitative Health Sciences, Cleveland Clinic, Cleveland, OH, USA.
Brain Commun. 2021 Jul 16;3(3):fcab164. doi: 10.1093/braincomms/fcab164. eCollection 2021.
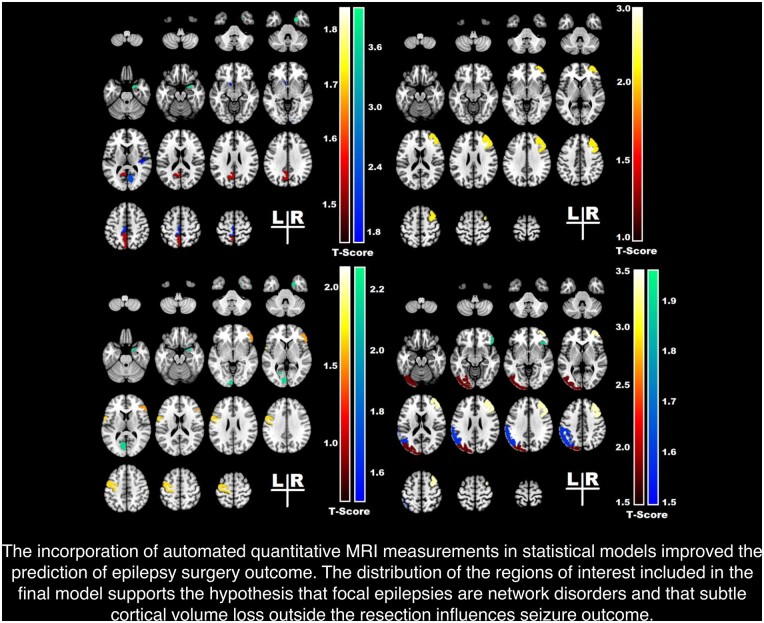
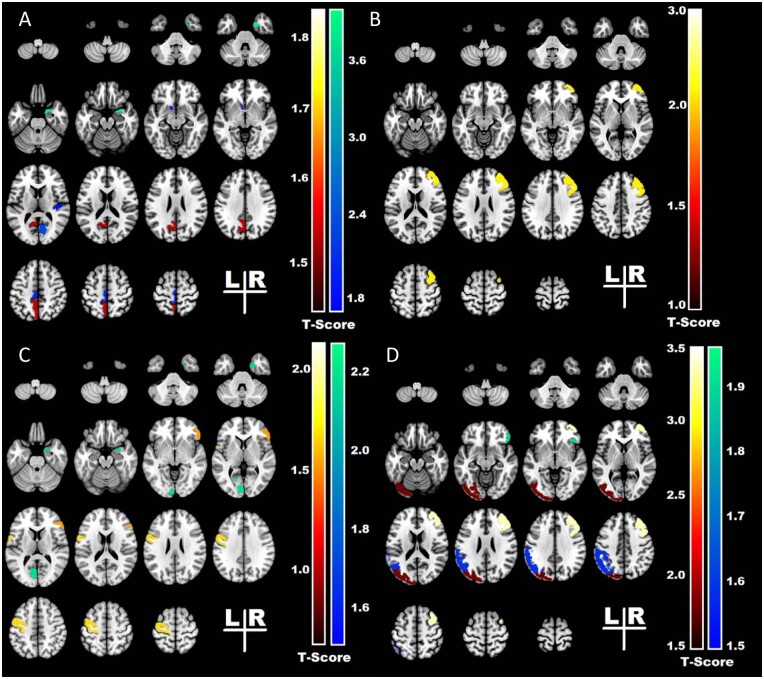
Quantitative volumetric brain MRI measurement is important in research applications, but translating it into patient care is challenging. We explore the incorporation of clinical automated quantitative MRI measurements in statistical models predicting outcomes of surgery for temporal lobe epilepsy. Four hundred and thirty-five patients with drug-resistant epilepsy who underwent temporal lobe surgery at Cleveland Clinic, Mayo Clinic and University of Campinas were studied. We obtained volumetric measurements from the pre-operative T1-weighted MRI using NeuroQuant, a Food and Drug Administration approved software package. We created sets of statistical models to predict the probability of complete seizure-freedom or an Engel score of I at the last follow-up. The cohort was randomly split into training and testing sets, with a ratio of 7:3. Model discrimination was assessed using the concordance statistic (C-statistic). We compared four sets of models and selected the one with the highest concordance index. Volumetric differences in pre-surgical MRI located predominantly in the frontocentral and temporal regions were associated with poorer outcomes. The addition of volumetric measurements to the model with clinical variables alone increased the model's C-statistic from 0.58 to 0.70 (right-sided surgery) and from 0.61 to 0.66 (left-sided surgery) for complete seizure freedom and from 0.62 to 0.67 (right-sided surgery) and from 0.68 to 0.73 (left-sided surgery) for an Engel I outcome score. 57% of patients with extra-temporal abnormalities were seizure-free at last follow-up, compared to 68% of those with no such abnormalities (-value = 0.02). Adding quantitative MRI data increases the performance of a model developed to predict post-operative seizure outcomes. The distribution of the regions of interest included in the final model supports the notion that focal epilepsies are network disorders and that subtle cortical volume loss outside the surgical site influences seizure outcome.
定量脑容积磁共振成像测量在研究应用中很重要,但将其应用于患者护理具有挑战性。我们探讨了将临床自动定量磁共振成像测量纳入预测颞叶癫痫手术结果的统计模型中。对在克利夫兰诊所、梅奥诊所和坎皮纳斯大学接受颞叶手术的435例耐药性癫痫患者进行了研究。我们使用美国食品药品监督管理局批准的软件包NeuroQuant,从术前T1加权磁共振成像中获得容积测量值。我们创建了多组统计模型,以预测最后一次随访时完全无癫痫发作或恩格尔分级为I级的概率。该队列被随机分为训练集和测试集,比例为7:3。使用一致性统计量(C统计量)评估模型的辨别力。我们比较了四组模型,并选择了一致性指数最高的一组。术前磁共振成像中主要位于额中央和颞叶区域的容积差异与较差的手术结果相关。仅将容积测量值添加到包含临床变量的模型中,对于完全无癫痫发作,模型的C统计量从0.58增加到0.70(右侧手术),从0.61增加到0.66(左侧手术);对于恩格尔I级结果评分,从0.62增加到0.67(右侧手术),从0.68增加到0.73(左侧手术)。在最后一次随访时,57%有颞叶外异常的患者无癫痫发作,而无此类异常的患者为68%(P值=0.02)。添加定量磁共振成像数据可提高用于预测术后癫痫发作结果的模型的性能。最终模型中感兴趣区域的分布支持了局灶性癫痫是网络疾病这一观点,并且手术部位外的细微皮质体积损失会影响癫痫发作结果。