Leong Darryl P, Cosman Tammy, Alhussein Muhammad M, Kumar Tyagi Nidhi, Karampatos Sarah, Barron Carly C, Wright Douglas, Tandon Vikas, Magloire Patrick, Joseph Philip, Conen David, Devereaux P J, Ellis Peter M, Mukherjee Som D, Dhesy-Thind Sukhbinder
Department of Medicine, Hamilton Health Sciences and McMaster University, Hamilton, Ontario, Canada.
The Population Health Research Institute, Hamilton Health Sciences and McMaster University, Hamilton, Ontario, Canada.
JACC CardioOncol. 2019 Jul 17;1(1):1-10. doi: 10.1016/j.jaccao.2019.06.004. eCollection 2019 Sep.
This study sought to evaluate the safety of continuing trastuzumab in patients with human epidermal growth factor receptor-positive breast cancer who developed mild cardiotoxicity.
Cardiotoxicity is the most common dose-limiting toxicity associated with trastuzumab. Current standard of care is discontinuation of trastuzumab, which can lead to worse cancer outcomes. It is unknown whether it is safe to continue trastuzumab despite mild cardiotoxicity.
Patients were eligible for this phase I, prospective, single-arm trial if left ventricular ejection fraction (LVEF) was between 40% and the lower limit of normal or if it fell ≥15% from baseline. Participants were treated with angiotensin-converting enzyme (ACE) inhibitors and/or beta-blockers in a cardio-oncology clinic and were followed clinically and with serial echocardiograms for 1 year. The primary outcome was cardiac dose-limiting toxicity, defined as cardiovascular death, LVEF <40% together with any heart failure symptoms, or LVEF <35%.
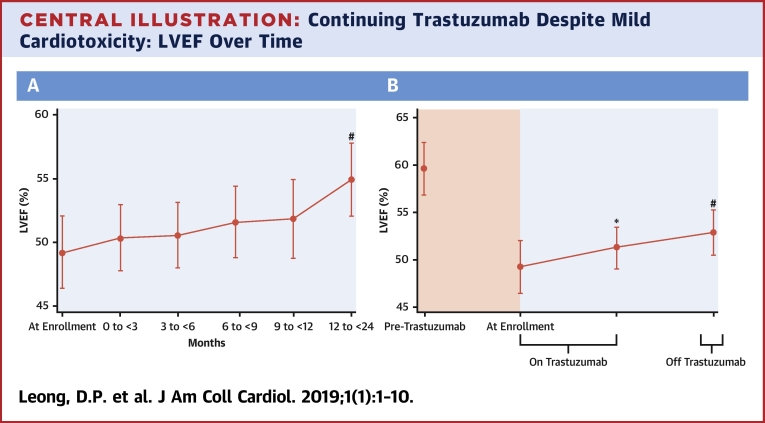
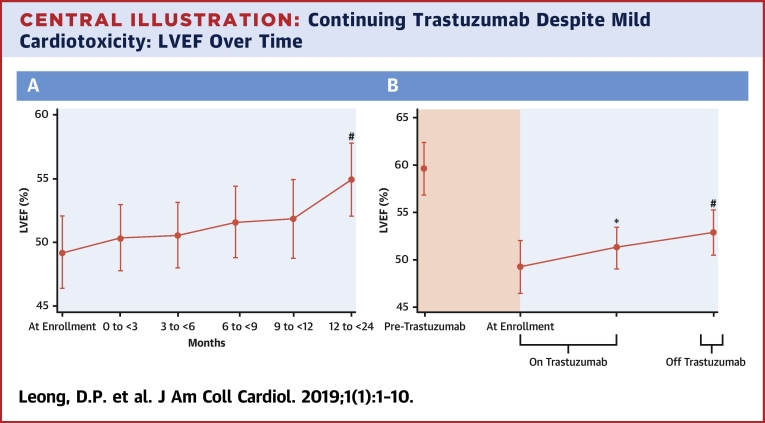
All 20 participants received ACE inhibitors and/or beta-blockers. A total of 18 participants (90%) received all planned trastuzumab doses. Two (10%) participants developed cardiac dose-limiting toxicity (heart failure with LVEF <40%). Their LVEF and heart failure symptoms improved to nearly normal following permanent trastuzumab discontinuation. There were no deaths. LVEF rose progressively from a mean of 49% at enrollment to 55% at 12 months (p < 0.001).
It may be feasible to continue trastuzumab despite mild cardiotoxicity in the setting of a cardio-oncology clinic, where ACE inhibitors and beta-blockers are administered. Approximately 10% of patients may develop moderate to severe heart failure using this approach. (Safety of Continuing Chemotherapy in Overt Left Ventricular Dysfunction Using Antibodies to Human Epidermal Growth Factor Receptor-2 [SCHOLAR]; NCT02907021).
本研究旨在评估在发生轻度心脏毒性的人表皮生长因子受体阳性乳腺癌患者中继续使用曲妥珠单抗的安全性。
心脏毒性是与曲妥珠单抗相关的最常见剂量限制性毒性。当前的标准治疗方案是停用曲妥珠单抗,这可能导致更差的癌症预后。尽管存在轻度心脏毒性,但继续使用曲妥珠单抗是否安全尚不清楚。
如果左心室射血分数(LVEF)在40%至正常下限之间,或者较基线下降≥15%,则患者有资格参加这项I期前瞻性单臂试验。参与者在心脏肿瘤门诊接受血管紧张素转换酶(ACE)抑制剂和/或β受体阻滞剂治疗,并接受临床随访和连续超声心动图检查1年。主要结局是心脏剂量限制性毒性,定义为心血管死亡、LVEF<40%并伴有任何心力衰竭症状,或LVEF<35%。
所有20名参与者均接受了ACE抑制剂和/或β受体阻滞剂治疗。共有18名参与者(90%)接受了所有计划的曲妥珠单抗剂量。两名(10%)参与者出现了心脏剂量限制性毒性(LVEF<40%的心力衰竭)。在永久性停用曲妥珠单抗后,他们的LVEF和心力衰竭症状改善至接近正常。无死亡病例。LVEF从入组时的平均49%逐渐升至12个月时的55%(p<0.001)。
在使用ACE抑制剂和β受体阻滞剂的心脏肿瘤门诊环境中,尽管存在轻度心脏毒性,但继续使用曲妥珠单抗可能是可行的。采用这种方法,约10%的患者可能会发生中度至重度心力衰竭。(使用抗人表皮生长因子受体-2抗体在明显左心室功能障碍中继续化疗的安全性[SCHOLAR];NCT02907021)