Division of Cardiology, Department of Internal Medicine, Keimyung University Dongsan Hospital, Keimyung University School of Medicine, Daegu, Republic of Korea.
Department of Radiology, Keimyung University School of Medicine, Keimyung University Dongsan Hospital, Daegu, Republic of Korea.
Medicine (Baltimore). 2021 Aug 6;100(31):e26702. doi: 10.1097/MD.0000000000026702.
Pulmonary vein isolation (PVI) is the cornerstone of atrial fibrillation (AF) catheter ablation. However, a PVI alone has been considered insufficient for persistent AF. This study aimed to evaluate the efficacy of persistent AF ablation targeting complex fractionated atrial electrogram (CFAE) areas within low voltage zones identified by high-resolution mapping in addition to the PVI.
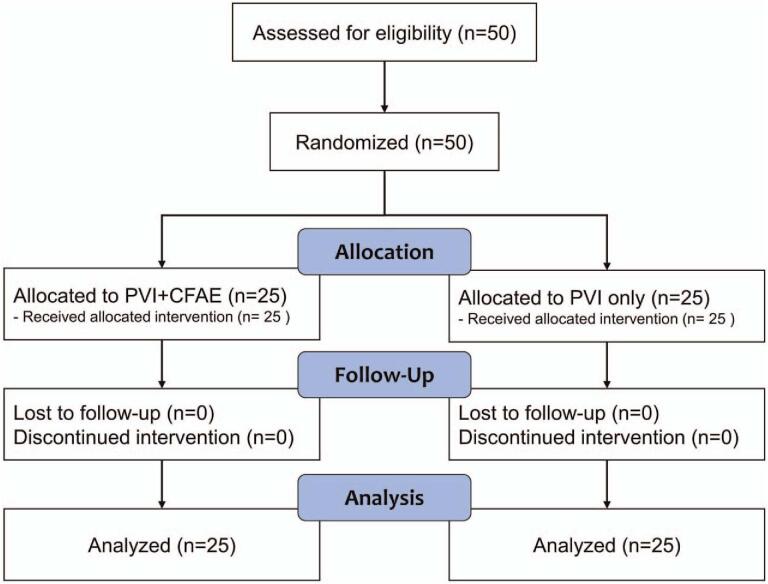
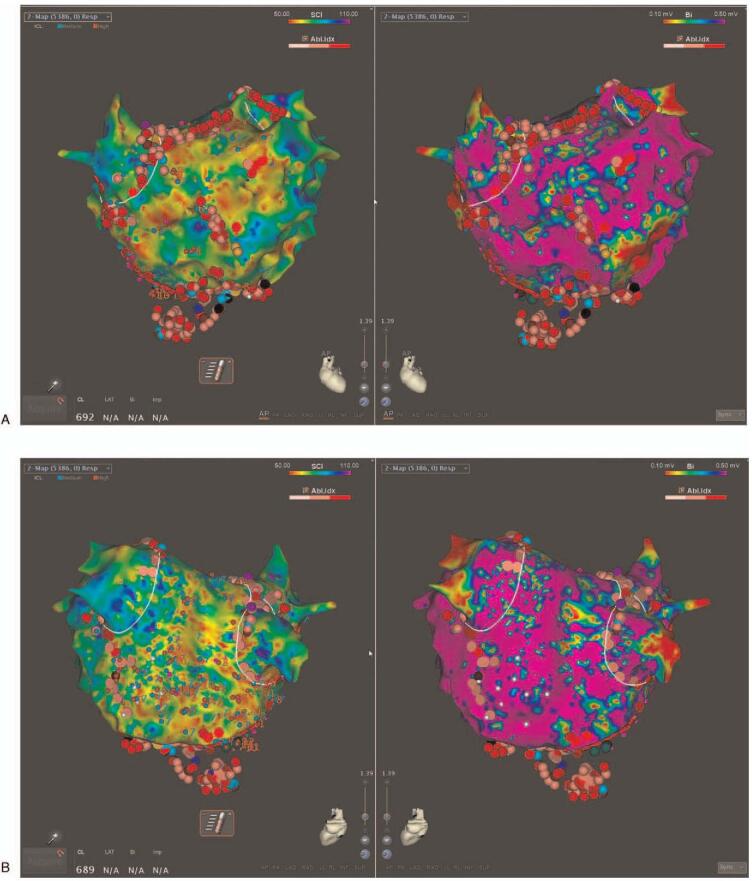
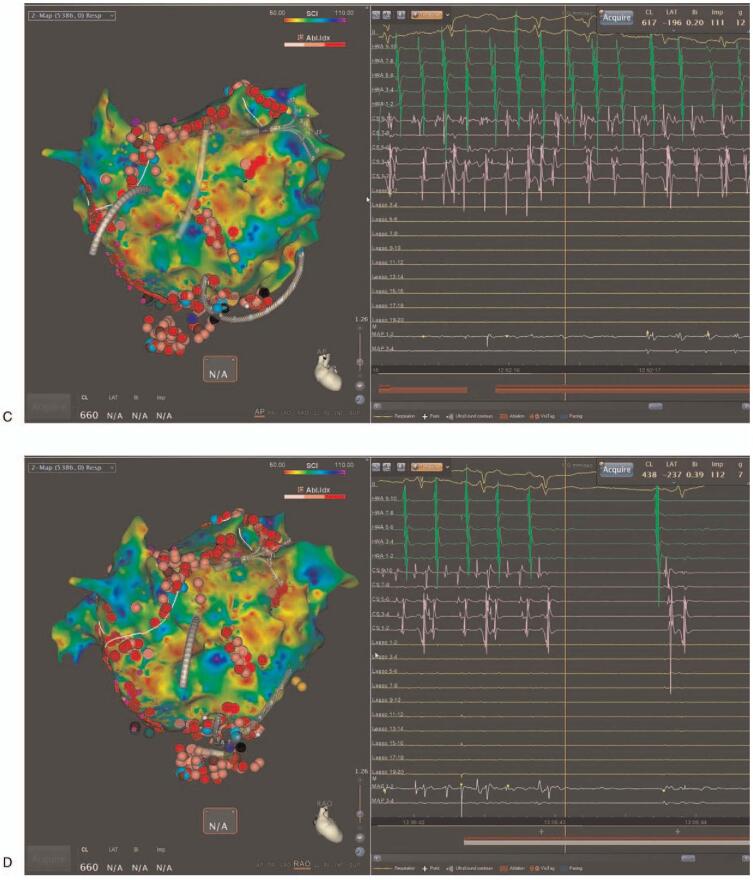
We randomized 50 patients (mean age 58.4 ± 9.5 years old, 86.0% males) with persistent AF to a PVI + CFAE group and PVI only group in a 1:1 ratio. CFAE and voltage mapping was performed simultaneously using a Pentaray Catheter with the CARTO3 CONFIDENSE module (Biosense Webster, CA, USA). The PVI + CFAE group, in addition to the PVI, underwent ablation targeting low voltage areas (<0.5 mV during AF) containing CFAEs.
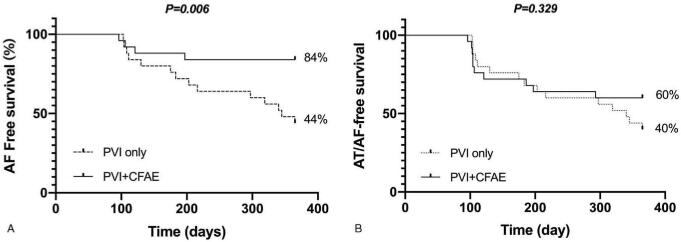
The mean persistent AF duration was 24.0 ± 23.1 months and mean left atrial dimension 4.9 ± 0.5 cm. In the PVI + CFAE group, AF converted to atrial tachycardia (AT) or sinus rhythm in 15 patients (60%) during the procedure. The PVI + CFAE group had a higher 1-year AF free survival (84.0% PVI + CFAE vs 44.0 PVI only, P = .006) without antiarrhythmic drugs. However, there was no difference in the AF/AT free survival (60.0% PVI + CFAE vs 40.0% PVI only, P = .329).
Persistent AF ablation targeting CFAE areas within low voltage zones using high-density voltage mapping had a higher AF free survival than a PVI only. Although recurrence with AT was frequent in the PVI+CFAE group, the sinus rhythm maintenance rate after redo procedures was 76%.
肺静脉隔离(PVI)是心房颤动(AF)导管消融的基石。然而,单独的 PVI 已被认为不足以治疗持续性 AF。本研究旨在评估在高分辨率标测识别的低电压区(存在碎裂心房电图(CFAE))内除 PVI 以外还针对 CFAE 区域进行持续性 AF 消融的疗效。
我们将 50 例(平均年龄 58.4±9.5 岁,男性占 86.0%)持续性 AF 患者随机分为 PVI+CFAE 组和 PVI 组,比例为 1:1。使用 Pentaray 导管和 CARTO3 CONFIDENSE 模块(Biosense Webster,CA,USA)同时进行 CFAE 和电压标测。除了 PVI 以外,PVI+CFAE 组还针对包含 CFAE 的低电压区(AF 期间<0.5mV)进行消融。
持续性 AF 平均时间为 24.0±23.1 个月,左心房内径平均为 4.9±0.5cm。在 PVI+CFAE 组,15 例患者(60%)在手术过程中转为房性心动过速(AT)或窦性心律。在未使用抗心律失常药物的情况下,PVI+CFAE 组 1 年 AF 无复发率(84.0% PVI+CFAE 比 44.0% PVI 组,P=0.006)更高。然而,AF/AT 无复发率无差异(60.0% PVI+CFAE 比 40.0% PVI 组,P=0.329)。
使用高密度电压标测在低电压区针对 CFAE 区域进行持续性 AF 消融比单纯 PVI 具有更高的 AF 无复发率。虽然 PVI+CFAE 组的复发率伴有 AT 较高,但在再次手术时的窦性心律维持率为 76%。