Department of Orthopaedic Surgery, University of Toledo Medical Center, 3065 Arlington Avenue, Toledo, OH, 43614, USA.
BMC Musculoskelet Disord. 2021 Aug 17;22(1):699. doi: 10.1186/s12891-021-04584-z.
Instrumented posterior lumbar fusion (IPLF) with and without transforaminal interbody fusion (TLIF) is a common treatment for low back pain when conservative interventions have failed. Certain patient comorbidities and lifestyle risk factors, such as obesity and smoking, are known to negatively affect these procedures. An advanced cellular bone allograft (CBA) with viable osteogenic cells (V-CBA) has demonstrated high fusion rates, but the rates for patients with severe and/or multiple comorbidities remain understudied. The purpose of this study was to assess fusion outcomes in patients undergoing IPLF/TLIF using V-CBA with baseline comorbidities and lifestyle risk factors known to negatively affect bone fusion.
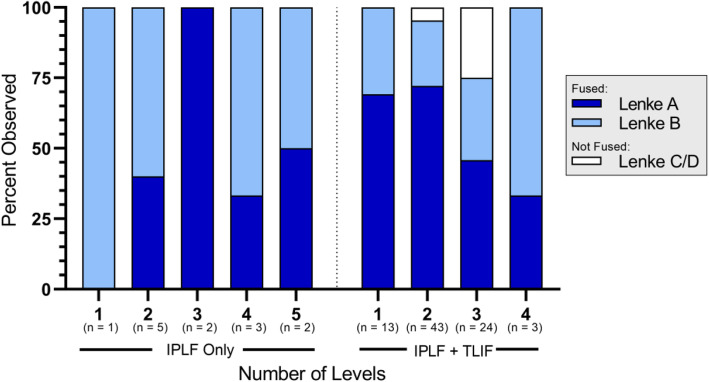
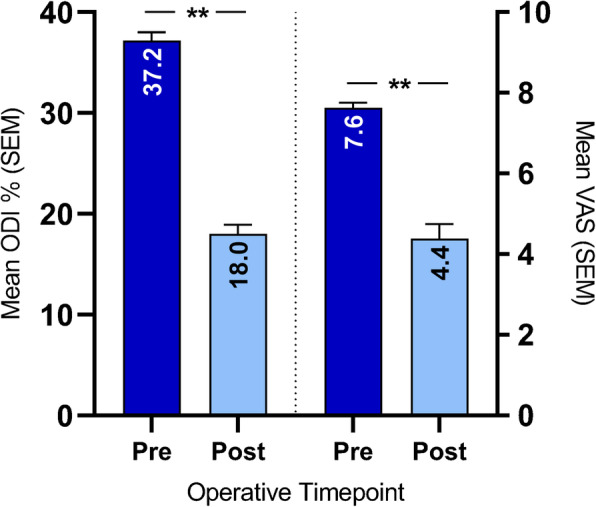
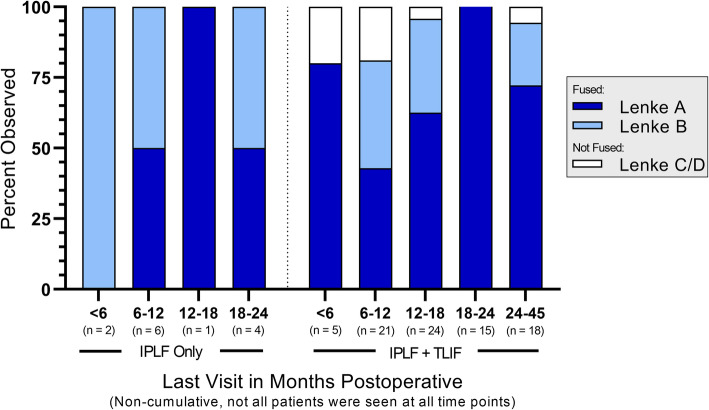
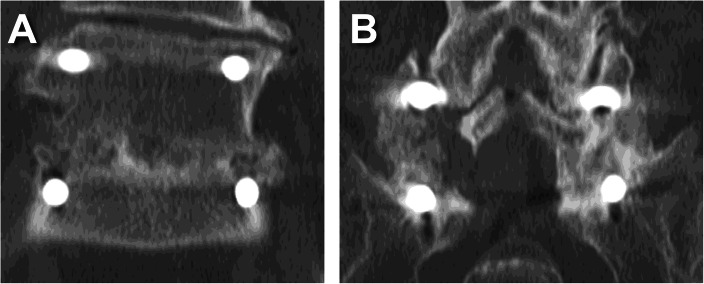
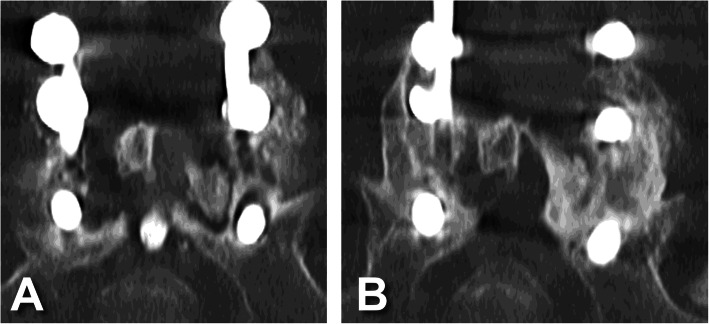
This was a retrospective study of de-identified data from consecutive patients at an academic medical center who underwent IPLF procedures with or without TLIF, and with V-CBA. Baseline patient and procedure characteristics were assessed. Radiological outcomes included fusion rates per the Lenke scale. Patient-reported clinical outcomes were evaluated via the Oswestry Disability Index (ODI) and Visual Analog Scale (VAS) for back and leg pain. Operating room (OR) times and intraoperative blood loss rates were also assessed.
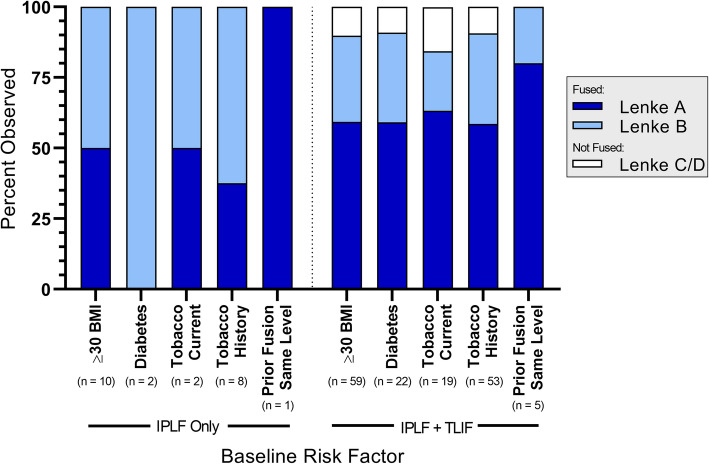
Data from 96 patients were assessed with a total of 222 levels treated overall (mean: 2.3 levels) and a median follow-up time of 16 months (range: 6 to 45 months). Successful fusion (Lenke A or B) was reported for 88 of 96 patients (91.7%) overall, including in all IPLF-only patients. Of 22 patients with diabetes in the IPLF+TLIF group, fusion was reported in 20 patients (90.9%). In IPLF+TLIF patients currently using tobacco (n = 19), fusion was reported in 16 patients (84.3%), while in those with a history of tobacco use (n = 53), fusion was observed in 48 patients (90.6%). Successful fusion was reported in all 6 patients overall with previous pseudarthrosis at the same level. Mean postoperative ODI and VAS scores were significantly reduced versus preoperative ratings.
The results of this study suggest that V-CBA consistently yields successful fusion and significant decreases in patient-reported ODI and VAS, despite patient comorbidities and lifestyle risk factors that are known to negatively affect such bony healing.
后路腰椎融合术(PLIF)联合或不联合经椎间孔腰椎间融合术(TLIF)是保守治疗失败后治疗腰痛的常用方法。某些患者合并症和生活方式风险因素,如肥胖和吸烟,已知会对这些手术产生负面影响。具有活成骨细胞的高级细胞骨移植物(CBA)已显示出较高的融合率,但在患有严重和/或多种合并症的患者中的融合率仍有待研究。本研究的目的是评估使用 V-CBA 治疗后路腰椎融合术(PLIF)/TLIF 患者的融合结果,这些患者存在已知会影响骨融合的基线合并症和生活方式风险因素。
这是一项回顾性研究,分析了来自学术医疗中心连续患者的匿名数据,这些患者接受了后路腰椎融合术(PLIF)联合或不联合 TLIF 手术,同时使用了 V-CBA。评估了基线患者和手术特征。影像学结果包括根据 Lenke 量表评估的融合率。通过 Oswestry 残疾指数(ODI)和腰背腿痛视觉模拟量表(VAS)评估患者报告的临床结果。还评估了手术室(OR)时间和术中失血量。
共评估了 96 名患者的数据,共治疗了 222 个节段(平均:2.3 个节段),中位随访时间为 16 个月(范围:6 至 45 个月)。96 名患者中有 88 名(91.7%)总体上报告了成功融合(Lenke A 或 B),包括所有仅接受 PLIF 治疗的患者。在接受 PLIF+TLIF 治疗的 22 名糖尿病患者中,20 名(90.9%)报告了融合。在目前正在吸烟的 19 名 PLIF+TLIF 患者中,16 名(84.3%)报告了融合,而在有吸烟史的 53 名患者中,48 名(90.6%)报告了融合。在同一水平上先前有假关节的 6 名患者总体上报告了成功融合。术后 ODI 和 VAS 评分与术前评分相比显著降低。
尽管患者合并症和生活方式风险因素已知会对骨愈合产生负面影响,但本研究结果表明,V-CBA 始终能产生成功的融合,并显著降低患者报告的 ODI 和 VAS。