Department of Research and Evaluation, Kaiser Permanente Southern California, Research and Evaluation, 100 S. Los Robles Avenue, 2nd Floor, Pasadena, CA, 91101, USA.
Kaiser Permanente Southern California, Regional Clinical Operations, Pasadena, USA.
BMC Health Serv Res. 2021 Aug 17;21(1):826. doi: 10.1186/s12913-021-06848-9.
Follow-up visits with clinic providers after hospital discharge may not be feasible for some patients due to functional limitations, transportation challenges, need for physical distancing, or fear of exposure especially during the current COVID-19 pandemic.
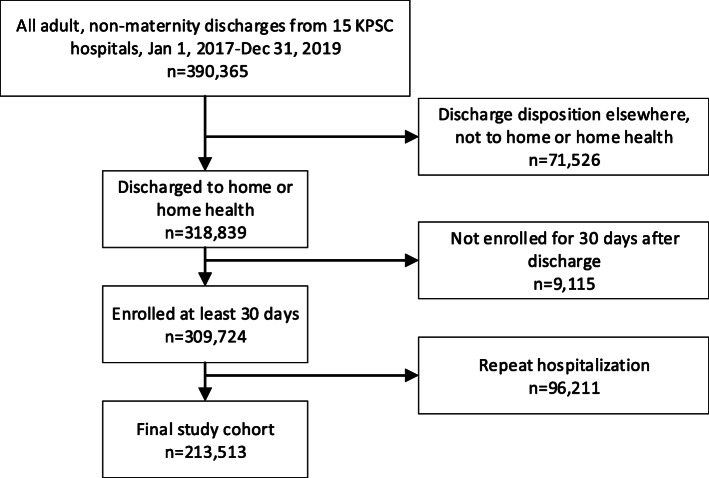
The aim of the study was to determine the effects of post-hospital clinic (POSH) and telephone (TPOSH) follow-up provider visits versus no visit on 30-day readmission. We used a retrospective cohort design based on data from 1/1/2017 to 12/31/2019 on adult patients (n = 213,513) discharged home from 15 Kaiser Permanente Southern California hospitals. Completion of POSH or TPOSH provider visits within 7 days of discharge was the exposure and all-cause 30-day inpatient and observation stay readmission was the primary outcome. We used matching weights to balance the groups and Fine-Gray subdistribution hazard model to assess for readmission risk.
Unweighted all-cause 30-day readmission rate was highest for patients who completed a TPOSH (17.3%) followed by no visit (14.2%), non-POSH (evaluation and management visits that were not focused on the hospitalization: 13.6%) and POSH (12.6%) visits. The matching weighted models showed that the effects of POSH and TPOSH visits varied across patient subgroups. For high risk (LACE 11+) medicine patients, both POSH (HR: 0.77, 95% CI: 0.71, 0.85, P < .001) and TPOSH (HR: 0.91, 95% CI: 0.83, 0.99, P = .03) were associated with 23 and 9% lower risk of 30-day readmission, respectively, compared to no visit. For medium to low risk medicine patients (LACE< 11) and all surgical patients regardless of LACE score or age, there were no significant associations for either visit type with risk of 30-day readmission.
Post-hospital telephone follow-up provider visits had only modest effects on 30-day readmission in high-risk medicine patients compared to clinic visits. It remains to be determined if greater use and comfort with virtual visits by providers and patients as a result of the pandemic might improve the effectiveness of these encounters.
由于功能限制、交通问题、物理距离需求或对感染的恐惧(尤其是在当前 COVID-19 大流行期间),对于一些患者而言,出院后与诊所医生的随访可能无法实现。
本研究的目的是确定医院后诊所(POSH)和电话(TPOSH)随访提供者就诊与不就诊对 30 天再入院的影响。我们使用了回顾性队列设计,基于 2017 年 1 月 1 日至 2019 年 12 月 31 日来自 15 家 Kaiser Permanente Southern California 医院出院回家的 213,513 名成年患者的数据。出院后 7 天内完成 POSH 或 TPOSH 就诊为暴露因素,全因 30 天住院和观察期再入院为主要结局。我们使用匹配权重来平衡组间差异,并使用 Fine-Gray 亚分布风险模型来评估再入院风险。
未加权的全因 30 天再入院率最高的是完成 TPOSH(17.3%)就诊的患者,其次是未就诊(14.2%)、非 POSH(非以住院为重点的评估和管理就诊:13.6%)和 POSH(12.6%)就诊的患者。匹配加权模型显示,POSH 和 TPOSH 就诊的效果在患者亚组中存在差异。对于高危(LACE 11+)药物患者,POSH(HR:0.77,95%CI:0.71,0.85,P<0.001)和 TPOSH(HR:0.91,95%CI:0.83,0.99,P=0.03)均与 30 天再入院风险降低 23%和 9%相关,与未就诊相比。对于中低危药物患者(LACE<11)和所有手术患者,无论 LACE 评分或年龄如何,两种就诊类型与 30 天再入院风险均无显著关联。
与诊所就诊相比,医院后电话随访提供者就诊对高危药物患者的 30 天再入院率仅有适度影响。由于大流行,提供者和患者对虚拟就诊的使用和舒适度是否会提高这些就诊的效果,还有待确定。