Infectious Diseases Department, Hospital Clinic de Barcelona, Barcelona, Spain.
Faculty of Medicine and Health Sciencies, University of Barcelona, Barcelona, Spain.
BMJ Open. 2021 Aug 17;11(8):e040775. doi: 10.1136/bmjopen-2020-040775.
Identifying undetected clinical signs is imperative in the prevention of SARS-CoV-2.
To establish the prevalence of clinical gustatory and olfactory dysfunctions in patients with COVID-19 pneumonia. Clinical outcomes and recovery rates associated with gustatory and olfactory dysfunctions were also assessed.
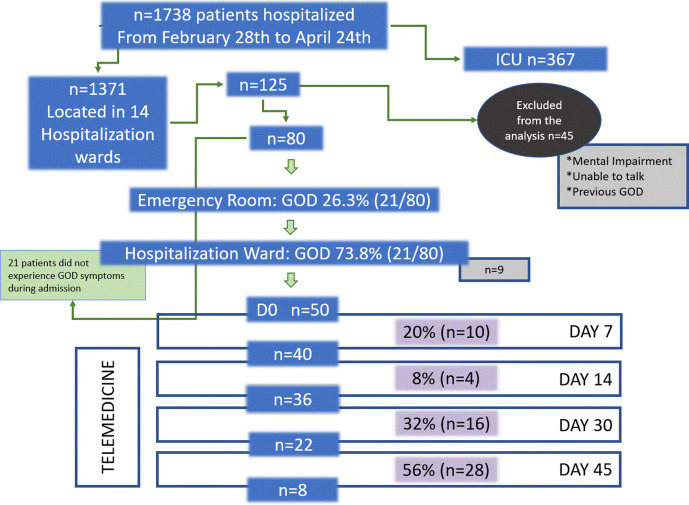
A prospective study was performed in 80 patients admitted to Hospital Clínic of Barcelona (Spain) for COVID-19 pneumonia. Patients were re-evaluated in the ward daily until discharge. Gustatory and olfactory dysfunction symptoms were retrospectively collected from emergency room (ER) charts after first assessments. Follow-up was performed in telemedicine consultation.
The single-centre study was performed in a hospitalisation ward at a university hospital.
Consecutive patients meeting hospitalisation criteria for COVID-19 pneumonia were eligible. Study exclusion criteria were patients who could not speak, had previous gustatory and olfactory dysfunctions or whose PCR tests for SARS-CoV-19 were negative.
Systematic assessment of gustatory and olfactory symptoms with standardised questions.
Prevalence of gustatory and olfactory dysfunctions in patients with COVID-19 pneumonia.
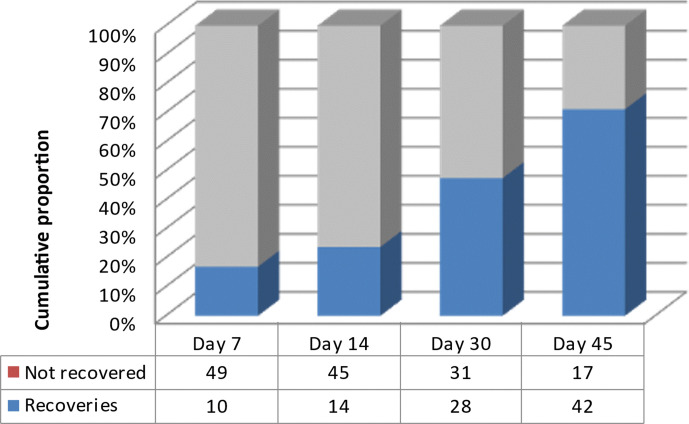
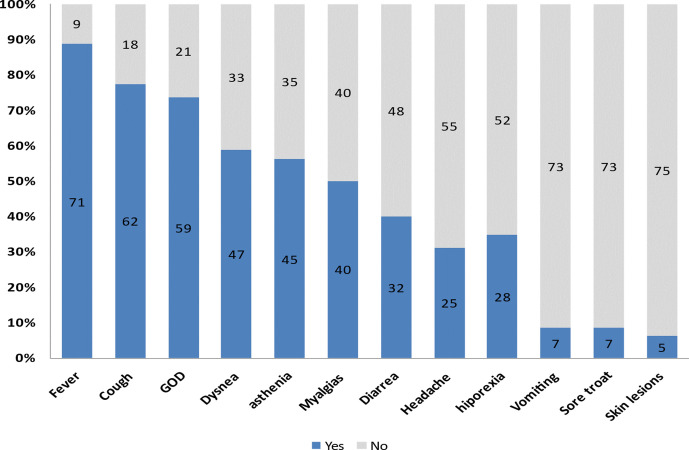
Of the 80 study subjects, 62.5% were male and the median age was 57 years. Half of the cohort (n=40) presented with comorbidities. The prevalence of chemosensitive disorder was 73.8% (n=59) (95% CI: 63.8 to 83.8), although self-reported symptoms were recorded in only 26.3% (n=21) of patients in the ER. Gustatory and olfactory dysfunctions were observed in 58.8% (n=47) and 55% (n=44) of cases, respectively. They were also the first symptoms in 25% (n=20) of patients. Anosmia was associated with ageusia, OR: 7, 95% CI: 2.3 to 21.8, p=0.001). No differences in clinical outcomes were observed when patients with and without gustatory and olfactory dysfunctions were compared. Recovery rates were 20% (n=10) and 85% (n=42) at days 7 and 45, respectively.
The prevalence of gustatory and olfactory dysfunctions in COVID-19 pneumonia was much higher than in self-report. Presence of gustatory and olfactory dysfunctions was not a predictor of clinical outcomes.
识别未被发现的临床症状对于预防 SARS-CoV-2 至关重要。
确定 COVID-19 肺炎患者味觉和嗅觉功能障碍的患病率。还评估了味觉和嗅觉功能障碍相关的临床结局和恢复率。
在巴塞罗那 Clinic 医院(西班牙)对 80 名因 COVID-19 肺炎住院的患者进行了前瞻性研究。在病房中每天对患者进行重新评估,直至出院。在首次评估后,从急诊室图表中回顾性收集味觉和嗅觉功能障碍症状。通过远程医疗咨询进行随访。
单中心研究在一所大学医院的住院病房进行。
符合 COVID-19 肺炎住院标准的连续患者有资格参加。研究排除标准为无法说话、有既往味觉和嗅觉障碍或 SARS-CoV-19 PCR 检测结果为阴性的患者。
使用标准化问题对味觉和嗅觉症状进行系统评估。
在 80 名研究对象中,62.5%为男性,中位年龄为 57 岁。一半的队列(n=40)有合并症。化学敏感障碍的患病率为 73.8%(n=59)(95%CI:63.8 至 83.8),尽管急诊科只有 26.3%(n=21)的患者记录了自述症状。味觉和嗅觉功能障碍分别在 58.8%(n=47)和 55%(n=44)的病例中观察到。它们也是 25%(n=20)患者的首发症状。嗅觉缺失与味觉缺失相关,OR:7,95%CI:2.3 至 21.8,p=0.001)。比较有和没有味觉和嗅觉功能障碍的患者时,临床结局没有差异。在第 7 天和第 45 天,恢复率分别为 20%(n=10)和 85%(n=42)。
COVID-19 肺炎患者味觉和嗅觉功能障碍的患病率远高于自述。味觉和嗅觉功能障碍的存在不是临床结局的预测因素。