Department of Data Science, Dana-Farber Cancer Institute, Boston, MA.
Department of Biostatistics, Harvard T. H. Chan School of Public Health, Boston, MA.
Blood. 2021 Dec 30;138(26):2810-2827. doi: 10.1182/blood.2020010146.
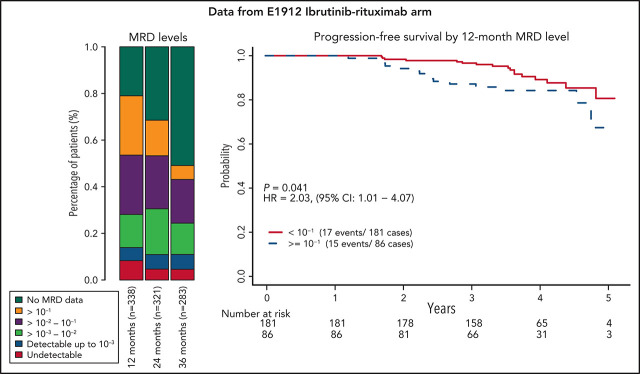
E1912 was a randomized phase 3 trial comparing indefinite ibrutinib plus 6 cycles of rituximab (IR) to 6 cycles of fludarabine, cyclophosphamide, and rituximab (FCR) in untreated younger patients with CLL. We describe measurable residual disease (MRD) levels in E1912 over time and correlate them with clinical outcome. Undetectable MRD rates (<1 CLL cell per 104 leukocytes) were 29.1%, 30.3%, 23.4%, and 8.6% at 3, 12, 24, and 36 months for FCR, and significantly lower at 7.9%, 4.2%, and 3.7% at 12, 24, and 36 months for IR, respectively. Undetectable MRD at 3, 12, 24, and 36 months was associated with longer progression-free survival (PFS) in the FCR arm, with hazard ratios (MRD detectable/MRD undetectable) of 4.29 (95% confidence interval [CI], 1.89-9.71), 3.91 (95% CI, 1.39-11.03), 14.12 (95% CI, 1.78-111.73), and not estimable (no events among those with undetectable MRD), respectively. In the IR arm, patients with detectable MRD did not have significantly worse PFS compared with those in whom MRD was undetectable; however, PFS was longer in those with MRD levels <10-1 than in those with MRD levels above this threshold. Our observations provide additional support for the use of MRD as a surrogate end point for PFS in patients receiving FCR. In patients on indefinite ibrutinib-based therapy, PFS did not differ significantly by undetectable MRD status, whereas those with MRD <10-1 tended to have longer PFS, although continuation of ibrutinib would very likely be necessary to maintain treatment efficacy.
E1912 是一项随机 3 期临床试验,比较了伊布替尼持续治疗与氟达拉滨、环磷酰胺和利妥昔单抗(FCR)6 个周期治疗在未经治疗的年轻 CLL 患者中的疗效。我们描述了 E1912 中随时间推移的可测量残留疾病(MRD)水平,并将其与临床结果相关联。FCR 组在 3、12、24 和 36 个月时的不可检测 MRD 率(每 104 个白细胞中有<1 个 CLL 细胞)分别为 29.1%、30.3%、23.4%和 8.6%,而伊布替尼组在 12、24 和 36 个月时的不可检测 MRD 率分别显著降低至 7.9%、4.2%和 3.7%。在 FCR 组中,3、12、24 和 36 个月时的不可检测 MRD 与更长的无进展生存期(PFS)相关,MRD 可检测/不可检测的危险比(HR)分别为 4.29(95%置信区间[CI],1.89-9.71)、3.91(95%CI,1.39-11.03)、14.12(95%CI,1.78-111.73)和不可估计(不可检测 MRD 者中无事件)。在伊布替尼组中,可检测到 MRD 的患者与不可检测到 MRD 的患者相比,PFS 无显著差异;然而,MRD 水平<10-1 的患者的 PFS 较长,而 MRD 水平高于该阈值的患者的 PFS 较短。我们的观察结果为将 MRD 作为接受 FCR 治疗的患者 PFS 的替代终点提供了额外的支持。在接受伊布替尼持续治疗的患者中,不可检测 MRD 状态对 PFS 无显著影响,而 MRD<10-1 的患者 PFS 更长,尽管为维持治疗效果很可能需要继续伊布替尼治疗。