Department of Health Care Policy, Harvard Medical School, Boston (Patel, Huskamp, Zubizarreta, Busch, Mehrotra); Division of General Medicine, Beth Israel Deaconess Medical Center, Boston (Mehrotra); Department of Medicine, Division of General Internal Medicine and Primary Care, Brigham and Women's Hospital, Boston (Barnett); Department of Health Policy and Management, Harvard T. H. Chan School of Public Health, Boston (Barnett); Department of Statistics, Harvard University, Cambridge (Zubizarreta); Department of Emergency Medicine, Massachusetts General Hospital, Boston (Zachrison); McLean Hospital, Belmont, Massachusetts (Busch); Department of Family Medicine, University of Vermont College of Medicine, Burlington (Wilcock).
Psychiatr Serv. 2022 Apr 1;73(4):403-410. doi: 10.1176/appi.ps.202100145. Epub 2021 Aug 19.
Because of limited access to psychiatrists, patients with acute mental illness in some emergency departments (EDs) may wait days for a consultation in the ED or as a medical-surgical admission. The study assessed whether telepsychiatry improves access to care and decreases ED wait times and hospital admissions.
ED visits with a primary diagnosis of mental illness were identified from 2010-2018 Medicare claims. A total of 134 EDs across 22 states that implemented telepsychiatry between 2013 and 2016 were matched 1:1 with control EDs without telepsychiatry on several characteristics, including availability of in-person psychiatrist consultations. Outcomes included patients' likelihood of admission to a medical-surgical or psychiatric bed, mental illness spending, prolonged ED length of stay (LOS) (two or more midnights in the ED), 90-day mortality, and outpatient follow-up care. Using a difference-in-difference design, changes in outcomes between the 3 years before telepsychiatry adoption and the 2 years after were examined.
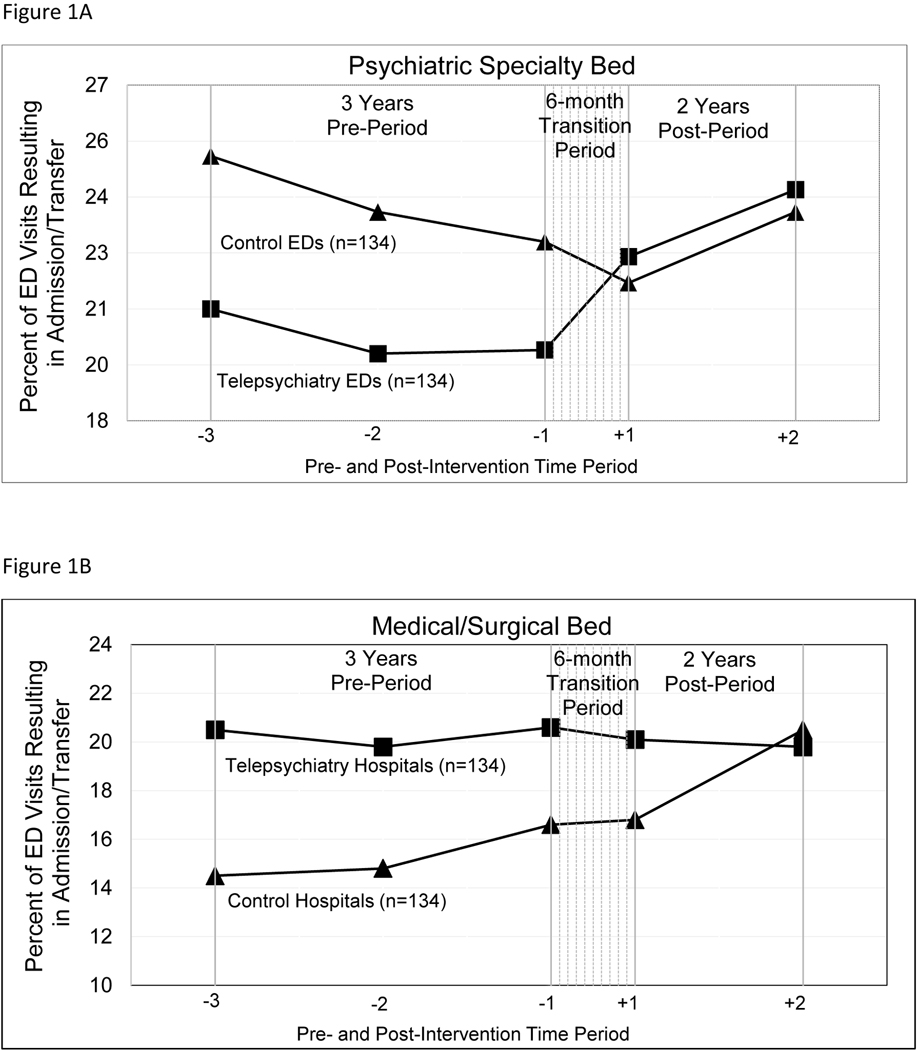
There were 172,708 ED mental illness visits across the 134 matched ED pairs in the study period. Telepsychiatry adoption was associated with increased admissions to a psychiatric bed (differential increase, 4.3 percentage points; p<0.001), decreased admissions to a medical-surgical bed (differential decrease, 2.0 percentage points; p<0.001), increased likelihood of a prolonged ED LOS (differential increase, 3.0 percentage points; p<0.001), and increased mental illness spending (differential increase, $292; p<0.01).
Telepsychiatry adoption was associated with a lower likelihood of admission to a medical-surgical bed but an increased likelihood of admission to a psychiatric bed and a prolonged ED LOS.
由于精神科医生资源有限,一些急诊科(ED)的急性精神疾病患者可能需要在 ED 等待数天才能获得咨询,或者作为内科-外科住院患者。本研究评估了远程精神病学是否可以改善患者的就诊机会,缩短 ED 等待时间和住院时间。
从 2010 年至 2018 年的医疗保险索赔中确定了以精神疾病为主要诊断的 ED 就诊。在 2013 年至 2016 年间实施远程精神病学的 22 个州的 134 家 ED 与没有远程精神病学的对照组 ED 进行了 1:1 匹配,这些 ED 在许多方面(包括是否有现场精神科医生咨询)具有相似性。结果包括患者被收治到内科-外科或精神科病床的可能性、精神疾病支出、延长 ED 住院时间(在 ED 度过两个或两个以上的午夜)、90 天死亡率和门诊随访情况。使用差异-差异设计,比较了远程精神病学采用前的 3 年和采用后的 2 年期间的结果变化。
在研究期间的 134 对匹配的 ED 中,共有 172708 例 ED 精神疾病就诊。采用远程精神病学后,收治到精神科病床的可能性增加(差异增加 4.3 个百分点;p<0.001),收治到内科-外科病床的可能性降低(差异降低 2.0 个百分点;p<0.001),ED 住院时间延长的可能性增加(差异增加 3.0 个百分点;p<0.001),精神疾病支出增加(差异增加 292 美元;p<0.01)。
采用远程精神病学后,收治到内科-外科病床的可能性降低,但收治到精神科病床和 ED 住院时间延长的可能性增加。