Department of Critical Care Medicine, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
Department of Critical Care Medicine, Zhejiang Hospital, Hangzhou, China.
Front Immunol. 2021 Aug 2;12:673693. doi: 10.3389/fimmu.2021.673693. eCollection 2021.
Thymosin alpha 1 (Tα1) is widely used to treat patients with COVID-19 in China; however, its efficacy remains unclear. This study aimed to explore the efficacy of Tα1 as a COVID-19 therapy.
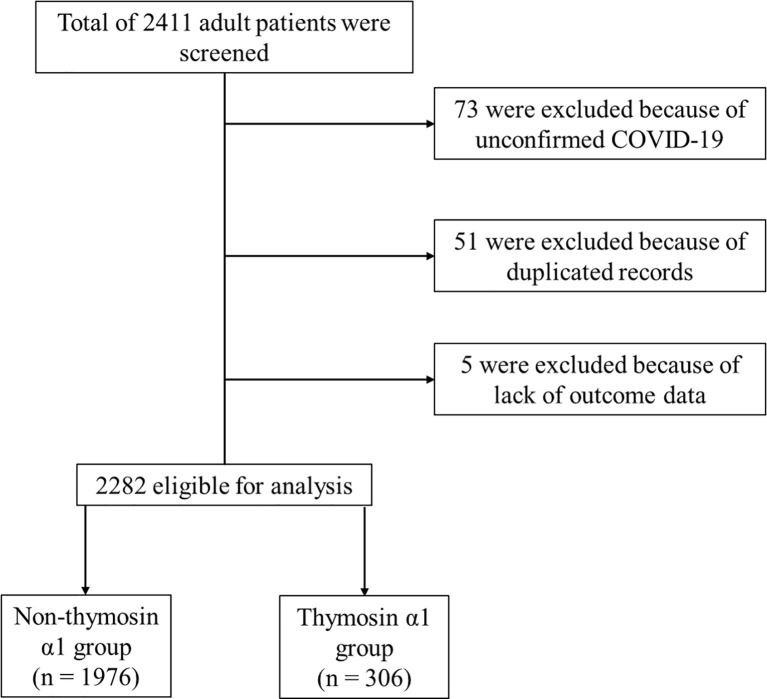
We performed a multicenter cohort study in five tertiary hospitals in the Hubei province of China between December 2019 and March 2020. The patient non-recovery rate was used as the primary outcome.
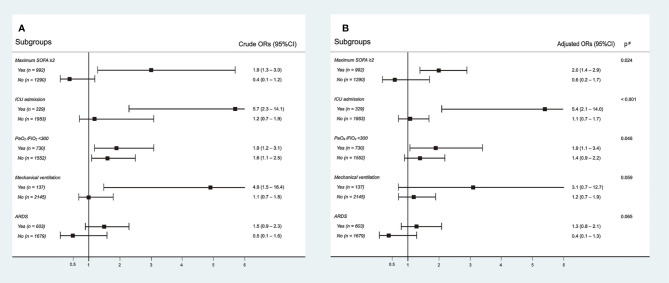
All crude outcomes, including non-recovery rate (65/306 290/1,976, = 0.003), in-hospital mortality rate (62/306 271/1,976, = 0.003), intubation rate (31/306 106/1,976, = 0.001), acute respiratory distress syndrome (ARDS) incidence (104/306 499/1,976, = 0.001), acute kidney injury (AKI) incidence (26/306 66/1,976, < 0.001), and length of intensive care unit (ICU) stay (14.9 ± 12.7 8.7 ± 8.2 days, < 0.001), were significantly higher in the Tα1 treatment group. After adjusting for confounding factors, Tα1 use was found to be significantly associated with a higher non-recovery rate than non-Tα1 use (OR 1.5, 95% CI 1.1-2.1, = 0.028). An increased risk of non-recovery rate associated with Tα1 use was observed in the patient subgroups with maximum sequential organ failure assessment (SOFA) scores ≥2 (OR 2.0, 95%CI 1.4-2.9, = 0.024), a record of ICU admission (OR 5.4, 95%CI 2.1-14.0, < 0.001), and lower PaO2/FiO2 values (OR 1.9, 95%CI 1.1-3.4, = 0.046). Furthermore, later initiation of Tα1 use was associated with a higher non-recovery rate.
Tα1 use in COVID-19 patients was associated with an increased non-recovery rate, especially in those with greater disease severity.
胸腺肽 α1(Tα1)在中国被广泛用于治疗 COVID-19 患者,但疗效仍不清楚。本研究旨在探讨 Tα1 作为 COVID-19 治疗方法的疗效。
我们在 2019 年 12 月至 2020 年 3 月期间在湖北省的五家三级医院进行了一项多中心队列研究。未恢复率被用作主要结局。
所有原始结局,包括未恢复率(65/306 290/1,976,=0.003)、住院死亡率(62/306 271/1,976,=0.003)、插管率(31/306 106/1,976,=0.001)、急性呼吸窘迫综合征(ARDS)发生率(104/306 499/1,976,=0.001)、急性肾损伤(AKI)发生率(26/306 66/1,976,<0.001)和 ICU 住院时间(14.9±12.7 8.7±8.2 天,<0.001),在 Tα1 治疗组中均显著更高。在调整混杂因素后,与非 Tα1 治疗相比,Tα1 使用与更高的未恢复率显著相关(OR 1.5,95%CI 1.1-2.1,=0.028)。在最大序贯器官衰竭评估(SOFA)评分≥2 的患者亚组(OR 2.0,95%CI 1.4-2.9,=0.024)、有 ICU 住院记录的患者亚组(OR 5.4,95%CI 2.1-14.0,<0.001)和 PaO2/FiO2 值较低的患者亚组(OR 1.9,95%CI 1.1-3.4,=0.046)中,Tα1 使用与未恢复率增加相关。此外,Tα1 起始时间较晚与未恢复率升高相关。
Tα1 在 COVID-19 患者中的使用与未恢复率升高相关,尤其是在病情较重的患者中。