Koroleva Ekaterina S, Kazakov Stanislav D, Tolmachev Ivan V, Loonen Anton J M, Ivanova Svetlana A, Alifirova Valentina M
Department of Neurology and Neurosurgery, Siberian State Medical University, 2 Moskovsky Trakt, 634050 Tomsk, Russia.
Department of Medical and Biological Cybernetics, Siberian State Medical University, 2 Moskovsky Trakt, 634050 Tomsk, Russia.
J Clin Med. 2021 Aug 21;10(16):3718. doi: 10.3390/jcm10163718.
Motor recovery after stroke is based on neuronal plasticity and the structural reorganization of the brain. Questions are debated about the proper moment to start rehabilitation in the acute period of stroke, the significance of rehabilitation interventions during the so-called "plastic window", and the advantages of modern and traditional programs. The aims of this study were to evaluate the role of different rehabilitation strategies and their combinations for motor recovery and the impact on functional disability by way of neurological and functional outcomes 3 months after ischemic stroke.
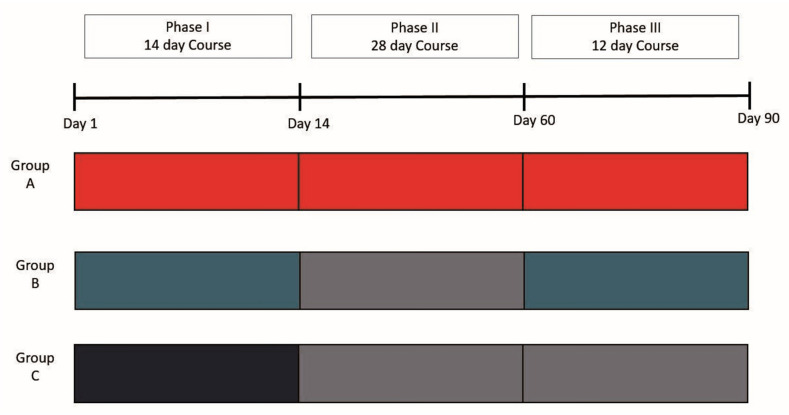
We used three rehabilitation approaches: early rehabilitation from the first day of stroke (Phase I), traditional exercise programs (Phase II), and an author's new method of biofeedback rehabilitation using motion sensors and augmented reality (AR) rehabilitation (Phase III). Clinical and functional outcomes were measured on the 90th day after stroke. We developed algorithms for quantifying the quality of movements during the execution of tasks in the motor domains of the AR rehabilitation program.
Phase I of rehabilitation led to an improvement in functional independence, and the recovery of motor functions of the extremities with an absence of mortality and clinical deterioration. AR rehabilitation led to significant improvement both with respect to clinical and functional scores on scales and to variables reflecting the quality of movements. Patients who were actively treated during Phases II and III achieved the same final level of motor recovery and functional outcomes as that of participants who had only received AR rehabilitation during Phase III. Patients who underwent outpatient observation after Phase I showed a deficit of spontaneous motor recovery on the 90th day after stroke.
Early rehabilitation was successful but was not enough; rehabilitation programs should be carried out throughout the entire "sensitive period" of poststroke plasticity. The newly developed AR biofeedback motion training is effective and safe as a separate rehabilitation method in the early recovery period of moderately severe, hemiparalytic, and ischemic stroke. These two rehabilitation approaches must be applied together or after each other, not instead of each other, as shown in clinical practice.
中风后的运动恢复基于神经元可塑性和大脑的结构重组。关于中风急性期开始康复的合适时机、所谓“可塑性窗口”期间康复干预的意义以及现代和传统方案的优势等问题仍存在争议。本研究的目的是通过缺血性中风后3个月的神经学和功能结果,评估不同康复策略及其组合对运动恢复的作用以及对功能残疾的影响。
我们采用了三种康复方法:从中风第一天开始的早期康复(第一阶段)、传统运动方案(第二阶段)以及作者使用运动传感器和增强现实(AR)康复的新型生物反馈康复方法(第三阶段)。在中风后第90天测量临床和功能结果。我们开发了用于量化AR康复计划运动领域任务执行过程中运动质量的算法。
第一阶段的康复导致功能独立性得到改善,四肢运动功能恢复,且无死亡率和临床恶化情况。AR康复在量表上的临床和功能评分以及反映运动质量的变量方面均有显著改善。在第二阶段和第三阶段积极接受治疗的患者与仅在第三阶段接受AR康复的参与者达到了相同的最终运动恢复水平和功能结果。在第一阶段后接受门诊观察的患者在中风后第90天显示出自发性运动恢复不足。
早期康复是成功的,但还不够;康复计划应在中风后可塑性的整个“敏感期”内进行实施。新开发的AR生物反馈运动训练作为中度严重、偏瘫和缺血性中风早期恢复期的一种独立康复方法是有效且安全的。在临床实践中,这两种康复方法必须一起应用或相继应用,而不是相互替代。