Zayed Military Hospital, Abu Dhabi, UAE.
Sheikh Khalifa Medical City, Abu Dhabi, UAE.
BMJ Open. 2021 Aug 26;11(8):e048770. doi: 10.1136/bmjopen-2021-048770.
To identify factors influencing the mortality risk in critically ill patients with COVID-19, and to develop a risk prediction score to be used at admission to intensive care unit (ICU).
A multicentre cohort study.
1542 patients with COVID-19 admitted to ICUs in public hospitals of Abu Dhabi, United Arab Emirates between 1 March 2020 and 22 July 2020.
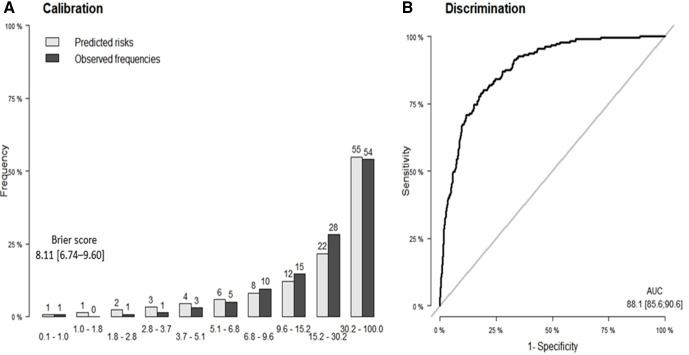
The primary outcome was time from ICU admission until death. We used competing risk regression models and Least Absolute Shrinkage and Selection Operator to identify the factors, and to construct a risk score. Predictive ability of the score was assessed by the area under the receiver operating characteristic curve (AUC), and the Brier score using 500 bootstraps replications.
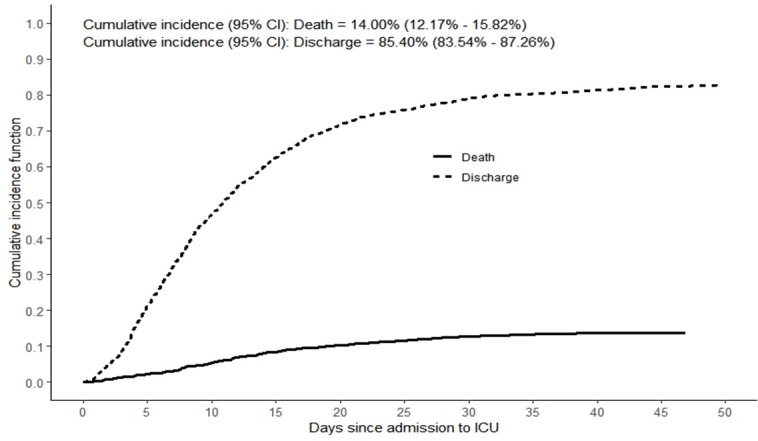
Among patients admitted to ICU, 196 (12.7%) died, 1215 (78.8%) were discharged and 131 (8.5%) were right-censored. The cumulative mortality incidence was 14% (95% CI 12.17% to 15.82%). From 36 potential predictors, we identified seven factors associated with mortality, and included in the risk score: age (adjusted HR (AHR) 1.98; 95% CI 1.71 to 2.31), neutrophil percentage (AHR 1.71; 95% CI 1.27 to 2.31), lactate dehydrogenase (AHR 1.31; 95% CI 1.15 to 1.49), respiratory rate (AHR 1.31; 95% CI 1.15 to 1.49), creatinine (AHR 1.19; 95% CI 1.11 to 1.28), Glasgow Coma Scale (AHR 0.70; 95% CI 0.63 to 0.78) and oxygen saturation (SpO) (AHR 0.82; 95% CI 0.74 to 0.91). The mean AUC was 88.1 (95% CI 85.6 to 91.6), and the Brier score was 8.11 (95% CI 6.74 to 9.60). We developed a freely available web-based risk calculator (https://icumortalityrisk.shinyapps.io/ICUrisk/).
In critically ill patients with COVID-19, we identified factors associated with mortality, and developed a risk prediction tool that showed high predictive ability. This tool may have utility in clinical settings to guide decision-making, and may facilitate the identification of supportive therapies to improve outcomes.
确定影响 COVID-19 重症患者死亡风险的因素,并开发一种风险预测评分,用于重症监护病房(ICU)入院时使用。
多中心队列研究。
2020 年 3 月 1 日至 2020 年 7 月 22 日期间,阿拉伯联合酋长国阿布扎比公立医院收治的 1542 例 COVID-19 患者入住 ICU。
主要结局是从 ICU 入院到死亡的时间。我们使用竞争风险回归模型和最小绝对收缩和选择算子来识别因素,并构建风险评分。通过 500 次 bootstrap 复制评估评分的预测能力,使用接收者操作特征曲线(AUC)下面积和 Brier 评分。
在入住 ICU 的患者中,196 人(12.7%)死亡,1215 人(78.8%)出院,131 人(8.5%)右删失。累积死亡率为 14%(95%CI 12.17%至 15.82%)。从 36 个潜在预测因素中,我们确定了 7 个与死亡率相关的因素,并纳入了风险评分:年龄(调整后的 HR(AHR)1.98;95%CI 1.71 至 2.31)、中性粒细胞百分比(AHR 1.71;95%CI 1.27 至 2.31)、乳酸脱氢酶(AHR 1.31;95%CI 1.15 至 1.49)、呼吸频率(AHR 1.31;95%CI 1.15 至 1.49)、肌酐(AHR 1.19;95%CI 1.11 至 1.28)、格拉斯哥昏迷量表(AHR 0.70;95%CI 0.63 至 0.78)和血氧饱和度(SpO)(AHR 0.82;95%CI 0.74 至 0.91)。平均 AUC 为 88.1(95%CI 85.6 至 91.6),Brier 评分 8.11(95%CI 6.74 至 9.60)。我们开发了一个免费的基于网络的风险计算器(https://icumortalityrisk.shinyapps.io/ICUrisk/)。
在 COVID-19 重症患者中,我们确定了与死亡率相关的因素,并开发了一种具有高预测能力的风险预测工具。该工具在临床环境中可能具有实用性,有助于指导决策,并可能有助于识别支持治疗以改善预后。